

A randomized controlled trial of directive and nondirective smoking cessation coaching through an employee quitline
- PMID: 27400966
- PMCID: PMC4940833
- DOI: 10.1186/s12889-016-3202-y
A randomized controlled trial of directive and nondirective smoking cessation coaching through an employee quitline
Abstract
Background: Telephone quitlines can help employees quit smoking. Quitlines typically use directive coaching, but nondirective, flexible coaching is an alternative. Call-2-Quit used a worksite-sponsored quitline to compare directive and nondirective coaching modes, and evaluated employee race and income as potential moderators.
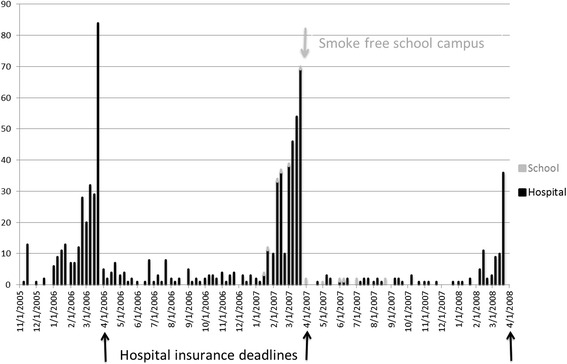
Methods: An unblinded randomized controlled trial compared directive and nondirective telephone coaching by trained laypersons. Participants were smoking employees and spouses recruited through workplace smoking cessation campaigns in a hospital system and affiliated medical school. Coaches were four non-medical women trained to use both coaching modes. Participants were randomized by family to coaching mode. Participants received up to 7 calls from coaches who used computer assisted telephone interview software to track topics and time. Outcomes were reported smoking abstinence for 7 days at last contact, 6 or 12 months after coaching began. Both worksites implemented new tobacco control policies during the study.
Results: Most participants responded to an insurance incentive introduced at the hospital. Call-2-Quit coached 518 participants: 22 % were African-American; 45 % had incomes below $30,000. Income, race, and intervention did not affect coaching completion rates. Cessation rates were comparable with directive and nondirective coaching (26 % versus 30 % quit, NS). A full factorial logistic regression model identified above median income (odds ratio = 1.8, p = 0.02), especially among African Americans (p = 0.04), and recent quit attempts (OR = 1.6, p = 0.03) as predictors of cessation. Nondirective coaching was associated with high cessation rates among subgroups of smokers reporting income above the median, recent quit attempts, or use of alternative therapies. Waiting up to 4 weeks to start coaching did not affect cessation. Of 41 highly addicted or depressed smokers who had never quit more than 30 days, none quit.
Conclusion: Nondirective coaching improved cessation rates for selected smoking employees, but less expensive directive coaching helped most smokers equally well, regardless of enrollment incentives and delays in receiving coaching. Some subgroups had very low cessation rates with either mode of quitline support.
Trial registration: ClinicalTrials.gov NCT02730260 , Registered March 31, 2016.
Keywords: Directive coaching; Employee health; Non-directive flexible coaching; Quitline; Smoking cessation.
Figures

References
-
- The Tobacco Use and Dependence Clinical Practice Guideline Panel, Staff, and Consortium Representatives. A clinical practice guideline for treating tobacco use and dependence: A US Public Health Service report. JAMA. 2000;283(24):3244-254. http://www.ncbi.nlm.nih.gov/pubmed/10866874?dopt=Citation - PubMed
-
- Stead LF, Lancaster T. Telephone counselling for smoking cessation. Cochrane Database Syst Rev. 2001;2:CD002850. - PubMed
-
- Fiore M, Jaén C, Baker T, Bailey W, Benowitz N, Curry S, Dorfman S, Froelicher E, Goldstein M, Healon C, et al. Clinical Practice Guideline. 2008/09/24 edn. Rockville: US Department of Health and Human Services. Public Health Service; 2008. Treating tobacco use and dependence: 2008 update; pp. 1217–1222.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
