

Role of ABC and Solute Carrier Transporters in the Placental Transport of Lamivudine
- PMID: 27401571
- PMCID: PMC4997848
- DOI: 10.1128/AAC.00648-16
Role of ABC and Solute Carrier Transporters in the Placental Transport of Lamivudine
Abstract
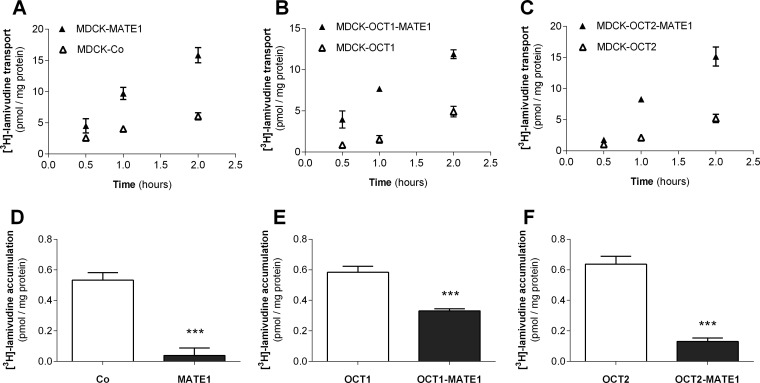
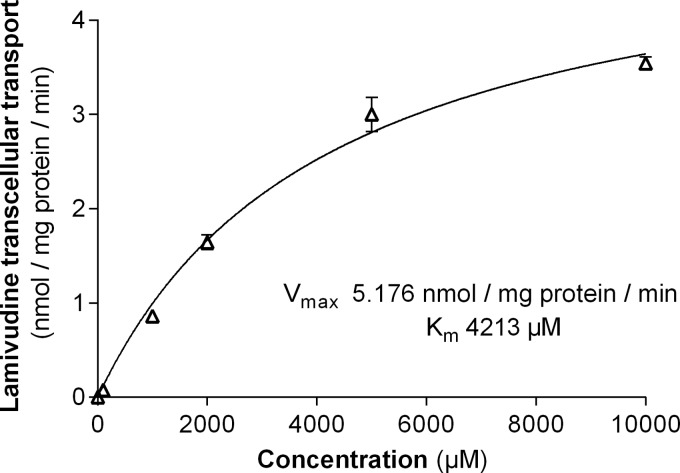
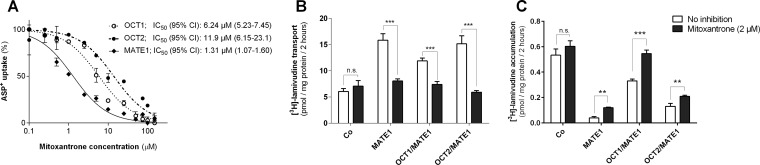
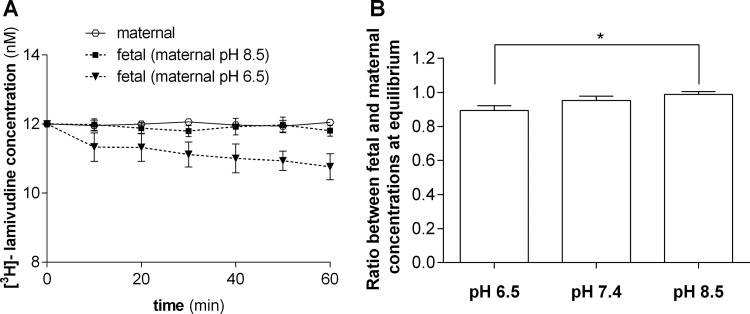
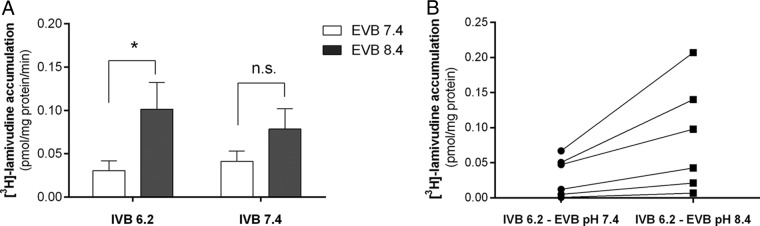
Lamivudine is one of the antiretroviral drugs of choice for the prevention of mother-to-child transmission (MTCT) in HIV-positive women. In this study, we investigated the relevance of drug efflux transporters P-glycoprotein (P-gp) (MDR1 [ABCB1]), BCRP (ABCG2), MRP2 (ABCC2), and MATE1 (SLC47A1) for the transmembrane transport and transplacental transfer of lamivudine. We employed in vitro accumulation and transport experiments on MDCK cells overexpressing drug efflux transporters, in situ-perfused rat term placenta, and vesicular uptake in microvillous plasma membrane (MVM) vesicles isolated from human term placenta. MATE1 significantly accelerated lamivudine transport in MATE1-expressing MDCK cells, whereas no transporter-driven efflux of lamivudine was observed in MDCK-MDR1, MDCK-MRP2, and MDCK-BCRP monolayers. MATE1-mediated efflux of lamivudine appeared to be a low-affinity process (apparent Km of 4.21 mM and Vmax of 5.18 nmol/mg protein/min in MDCK-MATE1 cells). Consistent with in vitro transport studies, the transplacental clearance of lamivudine was not affected by P-gp, BCRP, or MRP2. However, lamivudine transfer across dually perfused rat placenta and the uptake of lamivudine into human placental MVM vesicles revealed pH dependency, indicating possible involvement of MATE1 in the fetal-to-maternal efflux of the drug. To conclude, placental transport of lamivudine does not seem to be affected by P-gp, MRP2, or BCRP, but a pH-dependent mechanism mediates transport of lamivudine in the fetal-to-maternal direction. We suggest that MATE1 might be, at least partly, responsible for this transport.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- UNAIDS. 2015. Fact sheet 2014. Global statistics 2014; UNAIDS, Geneva, Switzerland: http://www.unaids.org/en/media/unaids/contentassets/documents/factsheet/....
-
- WHO. 2013. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach. World Health Organization, Geneva, Switzerland. - PubMed
-
- Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission. 2015. Recommendations for use of antiretroviral drugs in pregnant HIV-1-infected women for maternal health and interventions to reduce perinatal HIV transmission in the United States. http://aidsinfo.nih.gov/contentfiles/lvguidelines/PerinatalGL.pdf Accessed 26 May 2016.
-
- Wong F, Pai R, Van Schalkwyk J, Yoshida EM. 2014. Hepatitis B in pregnancy: a concise review of neonatal vertical transmission and antiviral prophylaxis. Ann Hepatol 13:187–195. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
