

The Substantial Loss of Nephrons in Healthy Human Kidneys with Aging
- PMID: 27401688
- PMCID: PMC5198286
- DOI: 10.1681/ASN.2016020154
The Substantial Loss of Nephrons in Healthy Human Kidneys with Aging
Abstract
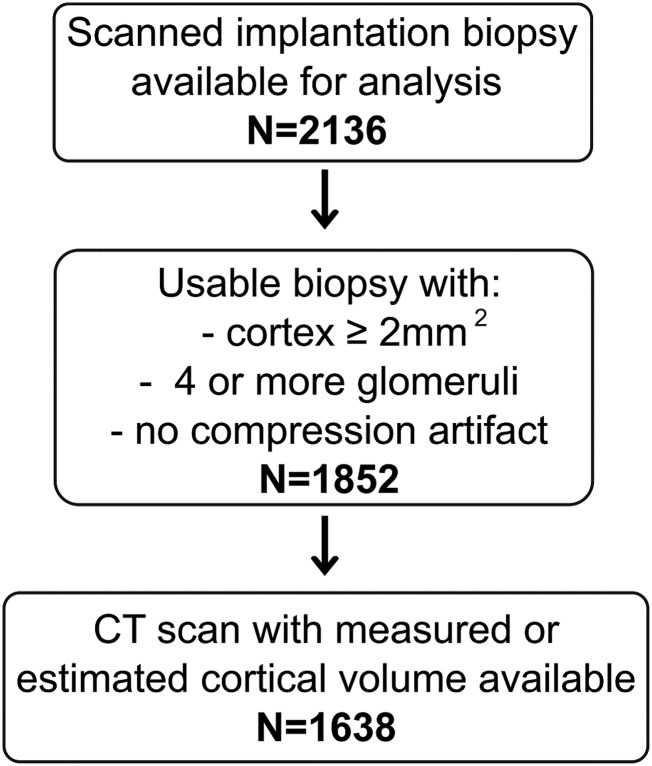
Nephron number may be an important determinant of kidney health but has been difficult to study in living humans. We evaluated 1638 living kidney donors at Mayo Clinic (MN and AZ sites) and Cleveland Clinic. We obtained cortical volumes of both kidneys from predonation computed tomography scans. At the time of kidney transplant, we obtained and analyzed the sections of a biopsy specimen of the cortex to determine the density of both nonsclerotic and globally sclerotic glomeruli; the total number of glomeruli was estimated from cortical volume×glomerular density. Donors 18-29 years old had a mean 990,661 nonsclerotic glomeruli and 16,614 globally sclerotic glomeruli per kidney, which progressively decreased to 520,410 nonsclerotic glomeruli per kidney and increased to 141,714 globally sclerotic glomeruli per kidney in donors 70-75 years old. Between the youngest and oldest age groups, the number of nonsclerotic glomeruli decreased by 48%, whereas cortical volume decreased by only 16% and the proportion of globally sclerotic glomeruli on biopsy increased by only 15%. Clinical characteristics that independently associated with fewer nonsclerotic glomeruli were older age, shorter height, family history of ESRD, higher serum uric acid level, and lower measured GFR. The incomplete representation of nephron loss with aging by either increased glomerulosclerosis or by cortical volume decline is consistent with atrophy and reabsorption of globally sclerotic glomeruli and hypertrophy of remaining nephrons. In conclusion, lower nephron number in healthy adults associates with characteristics reflective of both lower nephron endowment at birth and subsequent loss of nephrons.
Keywords: Aging; Nephron loss; Nephron number; kidney.
Copyright © 2016 by the American Society of Nephrology.
Figures



Comment in
-
Ageing: Nephron loss in the ageing kidney - it's more than you think.Nat Rev Nephrol. 2016 Oct;12(10):585-6. doi: 10.1038/nrneph.2016.130. Epub 2016 Aug 30. Nat Rev Nephrol. 2016. PMID: 27573729 No abstract available.
References
-
- Brenner BM, Garcia DL, Anderson S: Glomeruli and blood pressure. Less of one, more the other? Am J Hypertens 1: 335–347, 1988 - PubMed
-
- Hoy WE, Hughson MD, Bertram JF, Douglas-Denton R, Amann K: Nephron number, hypertension, renal disease, and renal failure. J Am Soc Nephrol 16: 2557–2564, 2005 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
