

The effects of respiratory sinus arrhythmia on anger reactivity and persistence in major depression
- PMID: 27401801
- PMCID: PMC5023471
- DOI: 10.1111/psyp.12722
The effects of respiratory sinus arrhythmia on anger reactivity and persistence in major depression
Abstract
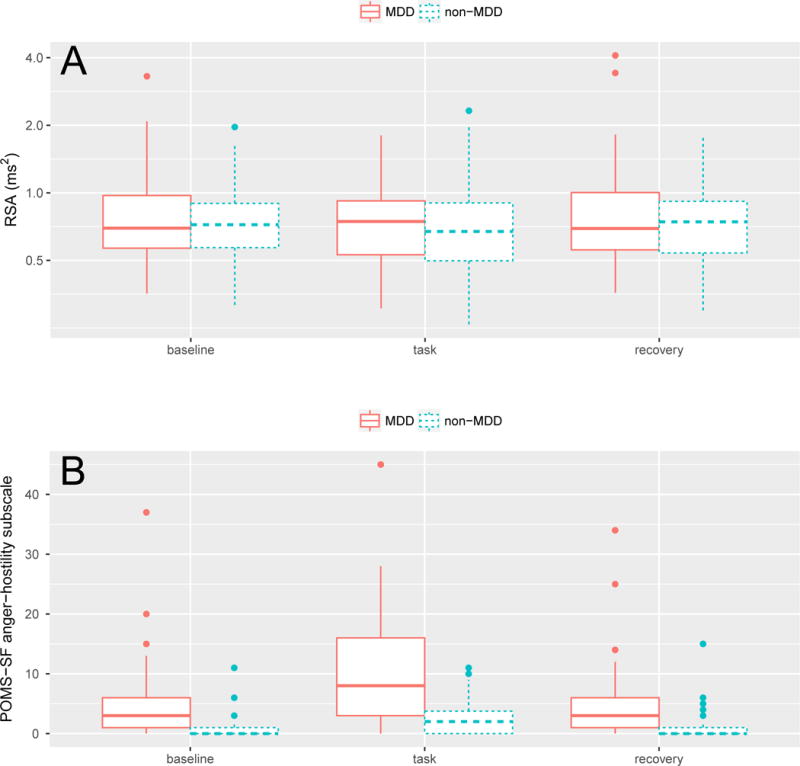
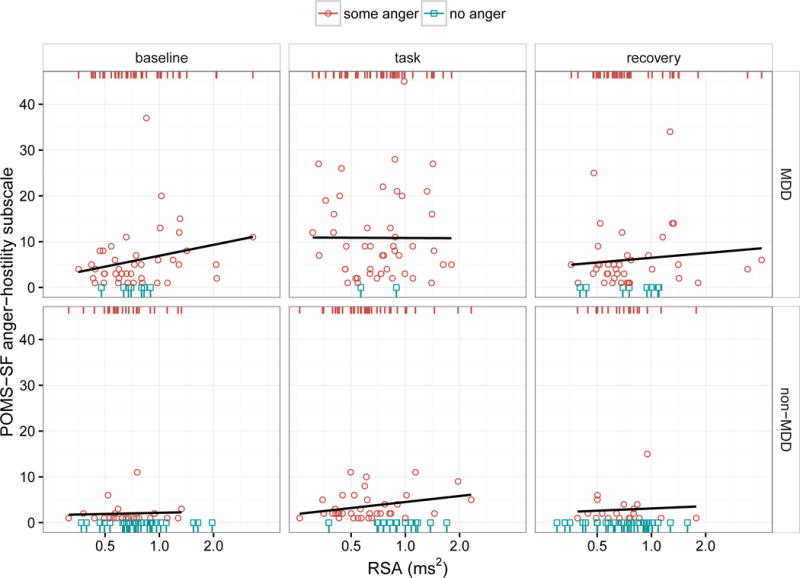
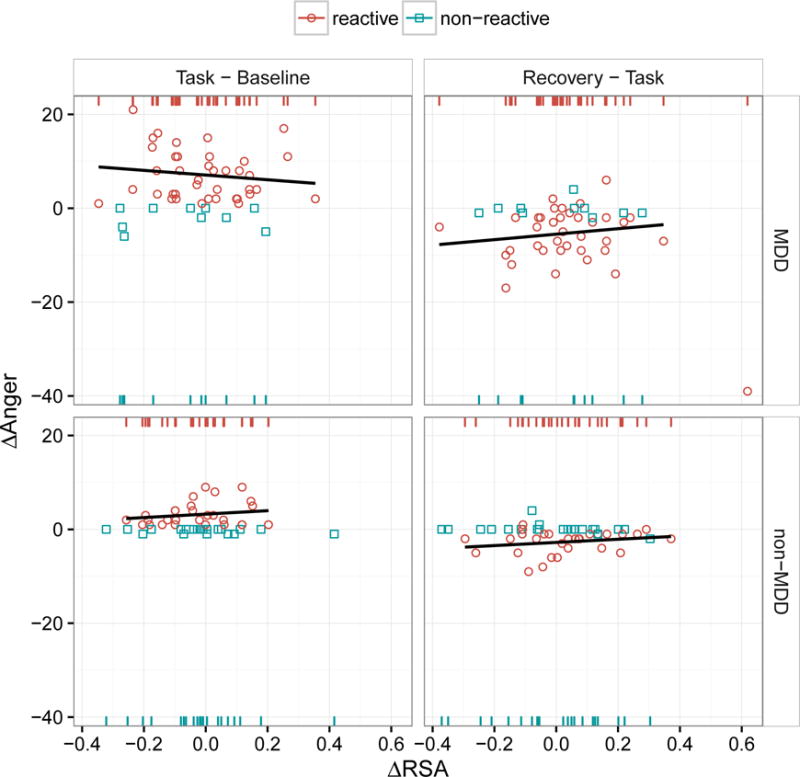
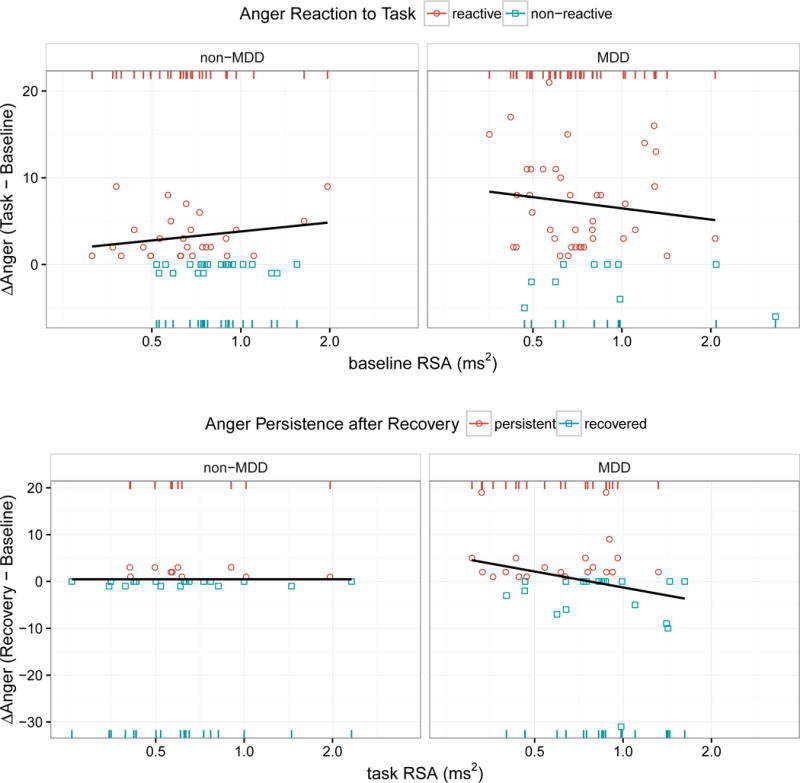
The experience of anger during a depressive episode has recently been identified as a poor prognostic indicator of illness course. Given the clinical implications of anger in major depressive disorder (MDD), understanding the mechanisms involved in anger reactivity and persistence is critical for improved intervention. Biological processes involved in emotion regulation during stress, such as respiratory sinus arrhythmia (RSA), may play a role in maintaining negative moods. Clinically depressed (MDD; n = 49) and nondepressed (non-MDD; n = 50) individuals were challenged with a stressful computer task shown to increase anger, while RSA (high frequency range 0.15-0.4 Hz) was collected. RSA predicted future anger, but was unrelated to current anger. That is, across participants, low baseline RSA predicted anger reactivity during the task, and in depressed individuals, those with low RSA during the task had a greater likelihood of anger persistence during a recovery period. These results suggest that low RSA may be a psychophysiological process involved in anger regulation in depression. Low RSA may contribute to sustained illness course by diminishing the repair of angry moods.
Keywords: Anger; Major depression; Mood persistence; Respiratory sinus arrhythmia.
© 2016 Society for Psychophysiological Research.
Figures
Similar articles
-
Respiratory sinus arrhythmia reactivity in current and remitted major depressive disorder.Psychosom Med. 2014 Jan;76(1):66-73. doi: 10.1097/PSY.0000000000000019. Epub 2013 Dec 23. Psychosom Med. 2014. PMID: 24367127 Free PMC article.
-
Respiratory sinus arrhythmia reactivity to a sad film predicts depression symptom improvement and symptomatic trajectory.Int J Psychophysiol. 2016 Jan;99:108-13. doi: 10.1016/j.ijpsycho.2015.12.002. Epub 2015 Dec 8. Int J Psychophysiol. 2016. PMID: 26681648 Free PMC article.
-
Respiratory sinus arrhythmia during worry forecasts stress-related increases in psychological distress.Stress. 2014 Sep;17(5):416-22. doi: 10.3109/10253890.2014.949666. Stress. 2014. PMID: 25089936
-
Respiratory sinus arrhythmia as a non-invasive index of 'brain-heart' interaction in stress.Indian J Med Res. 2016 Dec;144(6):815-822. doi: 10.4103/ijmr.IJMR_1447_14. Indian J Med Res. 2016. PMID: 28474618 Free PMC article. Review.
-
Heart rate and high frequency heart rate variability during stress as biomarker for clinical depression. A systematic review.Psychol Med. 2019 Jan;49(2):200-211. doi: 10.1017/S0033291718001988. Epub 2018 Aug 23. Psychol Med. 2019. PMID: 30134999
Cited by
-
Physiological Responses during Parental Conflicts as Potential Biomarkers for Adolescent Depression.Children (Basel). 2023 Jul 10;10(7):1195. doi: 10.3390/children10071195. Children (Basel). 2023. PMID: 37508692 Free PMC article.
-
Relationships between respiratory sinus arrhythmia and stress in college students.J Behav Med. 2020 Apr;43(2):308-317. doi: 10.1007/s10865-019-00103-7. Epub 2019 Oct 12. J Behav Med. 2020. PMID: 31606843 Free PMC article.
References
-
- Association, A. P. Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR (Text Revision) (Diagnostic & Statistical Manual of Mental Disorders (4 Sub) American Psychiatric Publishing, Inc; 2000.
-
- Beauchaine TP. Vagal tone, development, and Gray’s motivational theory: Toward an integrated model of autonomic nervous system functioning in psychopathology. Development and Psychopathology. 2001;13(2):183–214. http://doi.org/10.1017/S0954579401002012. - DOI - PubMed
-
- Beauchaine TP, Gatzke-Kopp L, Mead HK. Polyvagal Theory and developmental psychopathology: Emotion dysregulation and conduct problems from preschool to adolescence. Biological Psychology. 2007;74(2):174–184. http://doi.org/10.1016/j.biopsycho.2005.08.008. - DOI - PMC - PubMed
-
- Beck AT, Rial WY, Rickels K. Short form of Depression Inventory: Cross-validation. Psychological Reports. 1974;34(3, Pt 2):1184–1186. - PubMed
-
- Beck AT, Steer RA, Ball R, Ranieri WF. Comparison of Beck Depression Inventories–IA and –II in psychiatric outpatients. Journal of Personality Assessment. 1996;67(3):588–597. http://doi.org/10.1207/s15327752jpa6703_13. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
