

Sustained diffusion reversal with in-bore reperfusion in monkey stroke models: Confirmed by prospective magnetic resonance imaging
- PMID: 27401804
- PMCID: PMC5464696
- DOI: 10.1177/0271678X16659302
Sustained diffusion reversal with in-bore reperfusion in monkey stroke models: Confirmed by prospective magnetic resonance imaging
Abstract
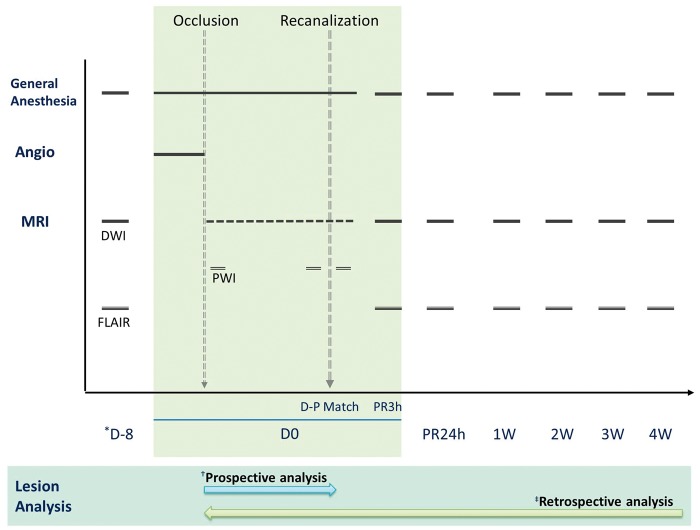
Although early diffusion lesion reversal after recanalization treatment of acute ischaemic stroke has been observed in clinical settings, the reversibility of lesions observed by diffusion-weighted imaging remains controversial. Here, we present consistent observations of sustained diffusion lesion reversal after transient middle cerebral artery occlusion in a monkey stroke model. Seven rhesus macaques were subjected to endovascular transient middle cerebral artery occlusion with in-bore reperfusion confirmed by repeated prospective diffusion-weighted imaging. Early diffusion lesion reversal was defined as lesion reversal at 3 h after reperfusion. Sustained diffusion lesion reversal was defined as the difference between the ADC-derived pre-reperfusion maximal ischemic lesion volume (ADCD-P Match) and the lesion on 4-week follow-up FLAIR magnetic resonance imaging. Diffusion lesions were spatiotemporally assessed using a 3-D voxel-based quantitative technique. The ADCD-P Match was 9.7 ± 6.0% (mean ± SD) and the final infarct was 1.2-6.0% of the volume of the ipsilateral hemisphere. Early diffusion lesion reversal and sustained diffusion lesion reversal were observed in all seven animals, and the calculated percentages compared with their ADCD-P Match ranged from 8.3 to 51.9% (mean ± SD, 26.9 ± 15.3%) and 41.7-77.8% (mean ± SD, 65.4 ± 12.2%), respectively. Substantial sustained diffusion lesion reversal and early reversal were observed in all animals in this monkey model of transient focal cerebral ischaemia.
Keywords: Animal model; brain imaging; brain ischaemia; brain recovery; diffusion-weighted magnetic resonance imaging.
Figures





References
-
- Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015; 372: 11–20. - PubMed
-
- Goyal M, Demchuk AM, Menon BK, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med 2015; 372: 1019–1030. - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med 2015; 372: 1009–1018. - PubMed
-
- Guadagno JV, Warburton EA, Jones PS, et al. The diffusion-weighted lesion in acute stroke: heterogeneous patterns of flow/metabolism uncoupling as assessed by quantitative positron emission tomography. Cerebrovasc Dis 2005; 19: 239–246. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
