

Management of Adverse Events Following Treatment With Anti-Programmed Death-1 Agents
- PMID: 27401894
- PMCID: PMC5061539
- DOI: 10.1634/theoncologist.2016-0055
Management of Adverse Events Following Treatment With Anti-Programmed Death-1 Agents
Abstract
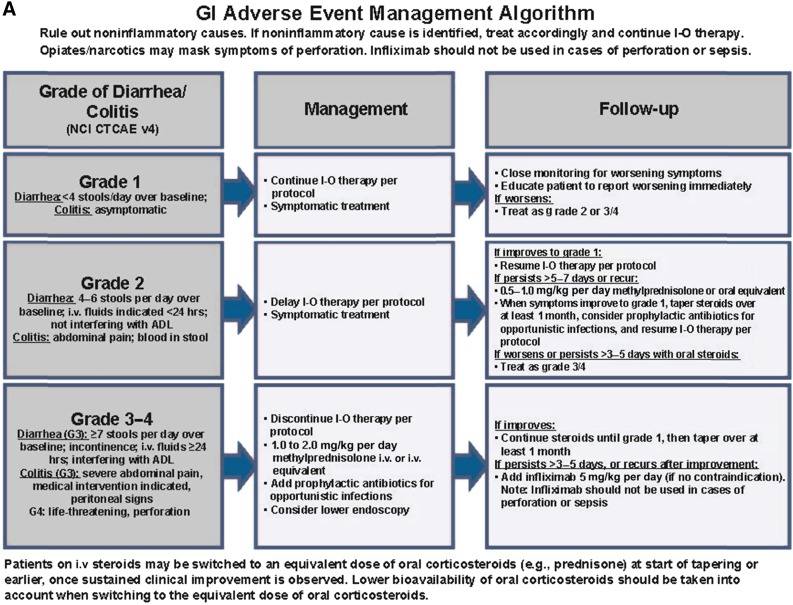
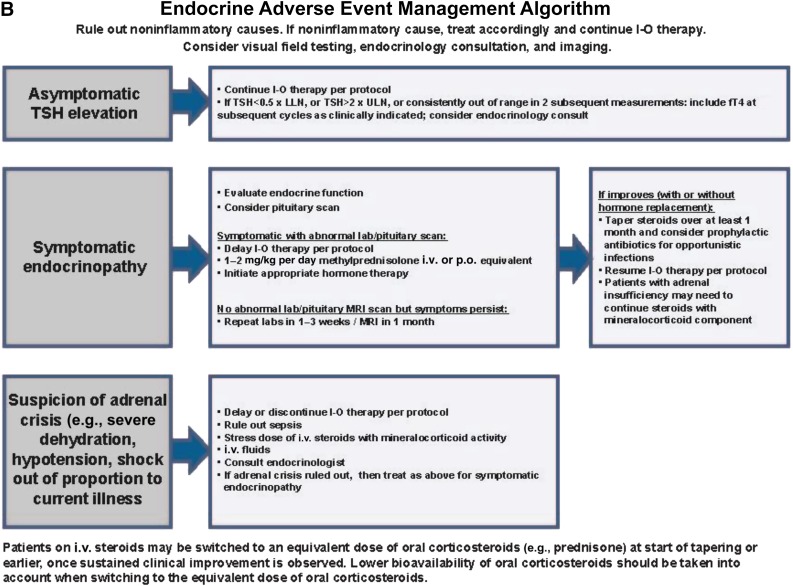
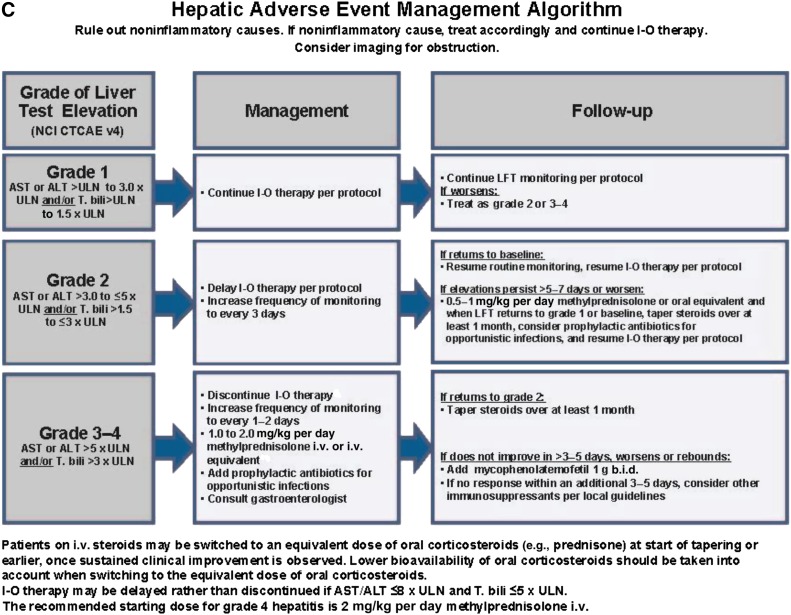
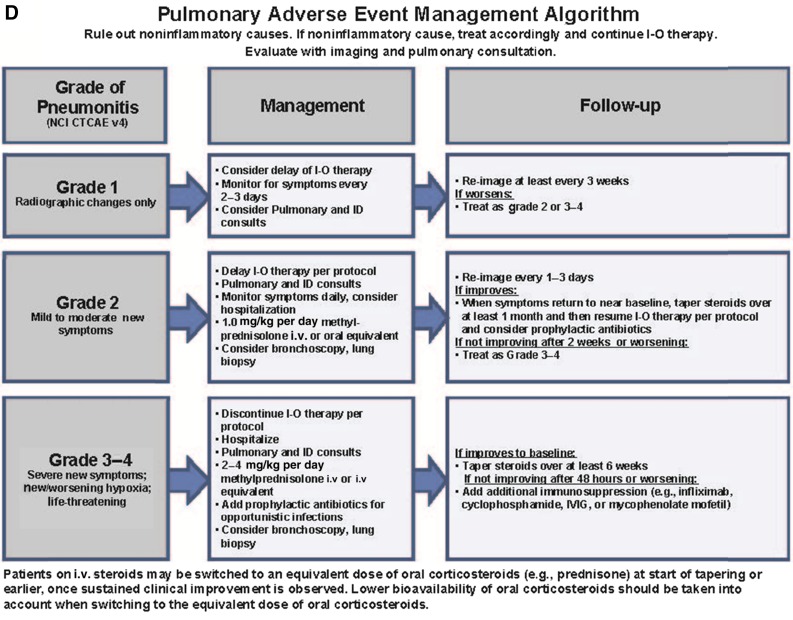
: Immune checkpoint inhibitors have emerged as a mainstay of melanoma therapy and are playing an increasingly important role in the treatment of other tumor types. The clinical benefit afforded by these treatments can be accompanied by a unique spectrum of adverse events, called immune-related adverse events (irAEs), which reflect the drug's immune-based mechanism of action. IrAEs typically originate in the skin, gastrointestinal tract, liver, and endocrine system, although other organ systems may also be affected. This article provides an overview of irAEs associated with anti-programmed death-1 (anti-PD-1) antibodies (nivolumab and pembrolizumab) as monotherapy or in combination with anti-cytotoxic T-lymphocyte antigen-4 inhibition (ipilimumab), followed by a discussion of irAEs of special clinical interest based on the potential for morbidity, frequent steroid use, and inpatient admission. We review clinical trial data and provide recommendations on how to manage irAEs associated with anti-PD-1 agents based on clinical experience and established management guidelines. We further illustrate the practical considerations of managing irAEs by presenting three cases of immune-related toxicity in melanoma patients treated with nivolumab or pembrolizumab. A better understanding of the identification and management of irAEs will help inform health care providers about the risks associated with anti-PD-1 treatment, to ensure the safe and appropriate use of these important new treatments.
Implications for practice: Immune checkpoint inhibitors have demonstrated significant clinical benefit in advanced melanoma and other tumor types. These treatments are associated with immune-related adverse events (irAEs), which most commonly affect the skin and gastrointestinal tract, and, to a lesser extent, the liver, endocrine system, and other organs. This review focuses on the management of irAEs after treatment with anti-programmed death-1 (anti-PD-1) antibodies (nivolumab or pembrolizumab) as monotherapy or in combination with anti-cytotoxic T-lymphocyte antigen-4 inhibition (ipilimumab) in patients with advanced melanoma. A better understanding of the management of irAEs will help ensure the safe and appropriate use of anti-PD-1 agents in melanoma and other tumor types.
Keywords: Drug-related side effects and adverse reactions; Melanoma; Nivolumab; Pembrolizumab; Programmed cell death 1 receptor.
©AlphaMed Press.
Conflict of interest statement
of potential conflicts of interest may be found at the end of this article.
Figures
Similar articles
-
Endocrine-related adverse events associated with immune checkpoint blockade and expert insights on their management.Cancer Treat Rev. 2017 Jul;58:70-76. doi: 10.1016/j.ctrv.2017.06.002. Epub 2017 Jun 22. Cancer Treat Rev. 2017. PMID: 28689073 Review.
-
Cutaneous, gastrointestinal, hepatic, endocrine, and renal side-effects of anti-PD-1 therapy.Eur J Cancer. 2016 Jun;60:190-209. doi: 10.1016/j.ejca.2016.02.025. Epub 2016 Apr 13. Eur J Cancer. 2016. PMID: 27085692
-
Safety of pembrolizumab for the treatment of melanoma.Expert Opin Drug Saf. 2015 Jun;14(6):957-64. doi: 10.1517/14740338.2015.1021774. Epub 2015 Apr 30. Expert Opin Drug Saf. 2015. PMID: 25927979 Review.
-
Neurological, respiratory, musculoskeletal, cardiac and ocular side-effects of anti-PD-1 therapy.Eur J Cancer. 2016 Jun;60:210-25. doi: 10.1016/j.ejca.2016.02.024. Epub 2016 Apr 13. Eur J Cancer. 2016. PMID: 27084345
-
The Next Immune-Checkpoint Inhibitors: PD-1/PD-L1 Blockade in Melanoma.Clin Ther. 2015 Apr 1;37(4):764-82. doi: 10.1016/j.clinthera.2015.02.018. Epub 2015 Mar 29. Clin Ther. 2015. PMID: 25823918 Free PMC article. Review.
Cited by
-
Sarcoid-like reaction: a unique response to immunotherapy in malignant melanoma.BMJ Case Rep. 2021 May 28;14(5):e243723. doi: 10.1136/bcr-2021-243723. BMJ Case Rep. 2021. PMID: 34049896 Free PMC article.
-
Psoriasis de novo or exacerbation by PD-1 checkpoint inhibitors.An Bras Dermatol. 2024 May-Jun;99(3):425-432. doi: 10.1016/j.abd.2023.09.003. Epub 2024 Feb 21. An Bras Dermatol. 2024. PMID: 38388337 Free PMC article. Review.
-
Safety of combined PD-1 pathway inhibition and radiation therapy for non-small-cell lung cancer: A multicentric retrospective study from the GFPC.Cancer Med. 2018 Nov;7(11):5505-5513. doi: 10.1002/cam4.1825. Epub 2018 Oct 11. Cancer Med. 2018. PMID: 30311424 Free PMC article.
-
Ipilimumab induced digital vasculitis.J Immunother Cancer. 2018 Feb 12;6(1):12. doi: 10.1186/s40425-018-0321-2. J Immunother Cancer. 2018. PMID: 29433584 Free PMC article.
-
Management of adverse events related to checkpoint inhibition therapy.Memo. 2018;11(2):132-137. doi: 10.1007/s12254-018-0416-y. Epub 2018 Jun 12. Memo. 2018. PMID: 29983828 Free PMC article. Review.
References
-
- Robert C, Long GV, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. 2015;372:320–330. - PubMed
-
- Weber JS, D’Angelo SP, Minor D, et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): A randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015;16:375–384. - PubMed
-
- Robert C, Schachter J, Long GV, et al. Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med. 2015;372:2521–2532. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
