

Spinal Subdural Abscess Following Laminectomy for Symptomatic Stenosis: A Report of 2 Cases and Review of the Literature
- PMID: 27402228
- PMCID: PMC4944552
- DOI: 10.12659/ajcr.897463
Spinal Subdural Abscess Following Laminectomy for Symptomatic Stenosis: A Report of 2 Cases and Review of the Literature
Abstract
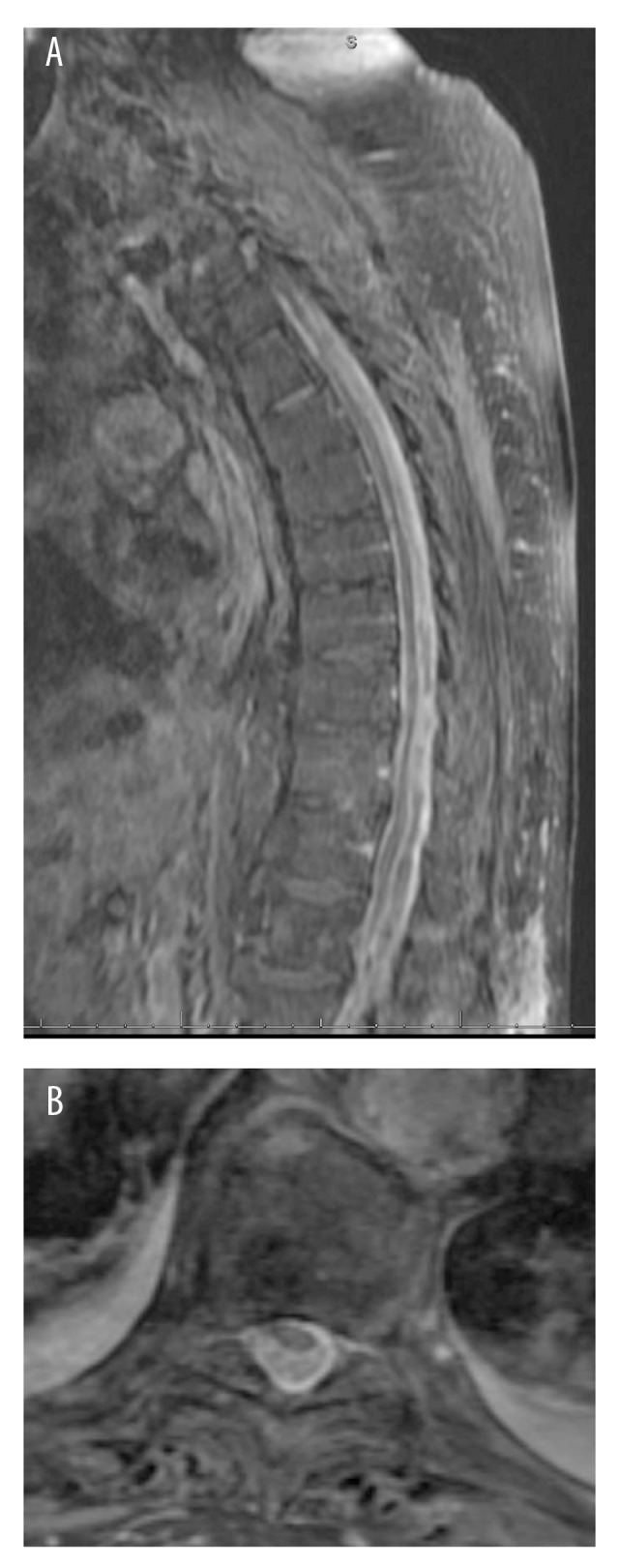
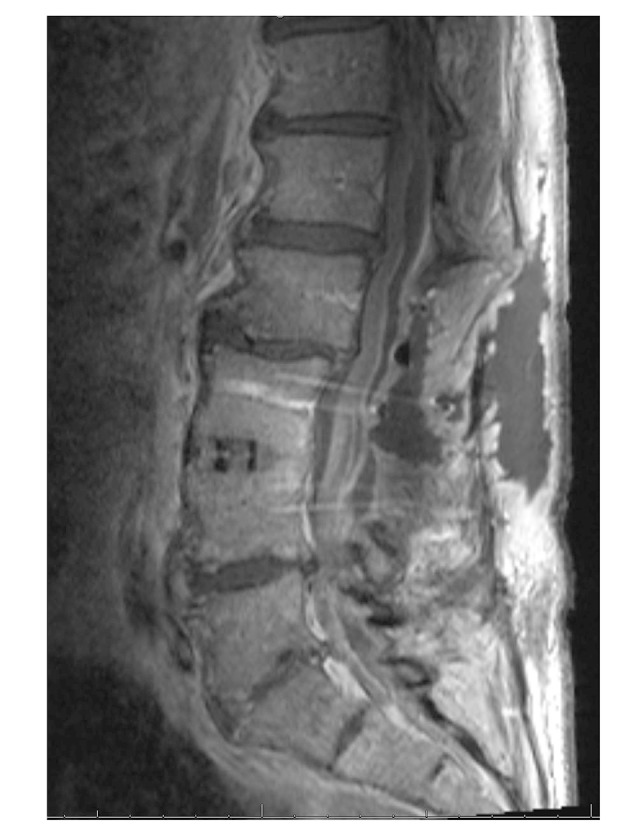
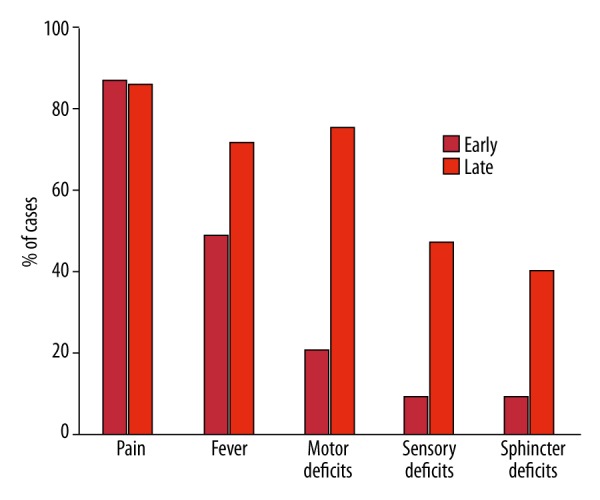
BACKGROUND Spinal subdural abscesses, also known as empyemas, are rare infectious lesions, the exact incidence of which is unknown. Presentation is typically dramatic, with back pain, fever, motor, and sensory deficits. Rapid identification and surgical intervention with laminectomy, durotomy, and washout provides the best outcomes. While hematogenous spread of an extra-spinal infection is the most common cause of this condition, a significant number of cases result from iatrogenic mechanisms, including lumbar punctures, epidural injections, and surgery. CASE REPORT Here we present 2 cases: 1) an 87-year-old man with type 2 diabetes, schizophrenia, mild cognitive impairment, and symptomatic lumbar spinal stenosis and 2) a 62-year-old man with a prior L3-4 spinal fusion with symptomatic lumbar spinal stenosis. In both cases, patients underwent laminectomy for spinal stenosis and developed epidural abscess. Following successful drainage of the epidural abscess, they continued to be symptomatic, and repeat imaging revealed the presence of a subdural abscess that was subsequently evacuated. Case 1 had significant improvement with residual lower-extremity weakness, while Case 2 made a complete neurological recovery. CONCLUSIONS These cases illustrate patients at increased risk for developing this rare spinal infection, and demonstrate that rapid recognition and surgical treatment is key to cure and recovery. Review of the literature highlights pertinent risk factors and demonstrates nearly one-third of reported cases have an iatrogenic etiology. The cases presented here demonstrate that a subdural process should be suspected in any patient with intractable pain following treatment of an epidural abscess.
Figures
References
-
- De Bonis P, Anile C, Pompucci A, et al. Cranial and spinal subdural empyema. Br J Neurosurg. 2009;23(3):335–40. - PubMed
-
- Abbott KH. Acute pyogenic spinal subdural abscess; A review of the literature and report of a case. Bull Los Angel Neuro Soc. 1940;18(2):91–102. - PubMed
-
- Abramovitz JN, Batson RA, Yablon JS. Vertebral osteomyelitis. The surgical management of neurologic complications. Spine. 1986;11(5):418–20. - PubMed
-
- Bartels RH, de Jong TR, Grotenhuis JA. Spinal subdural abscess. Case report. J Neurosurg. 1992;76(2):307–11. - PubMed
-
- Bennett AE, Keegan JJ. Circumscribed suppurations of the spinal cord and meninges. Report of a case of subdural abscess with functional recovery following operation. Arch Neurol Psychiatry. 1928;19:329–33.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
