

National Malaria Prevalence in Cambodia: Microscopy Versus Polymerase Chain Reaction Estimates
- PMID: 27402511
- PMCID: PMC5014264
- DOI: 10.4269/ajtmh.15-0908
National Malaria Prevalence in Cambodia: Microscopy Versus Polymerase Chain Reaction Estimates
Abstract
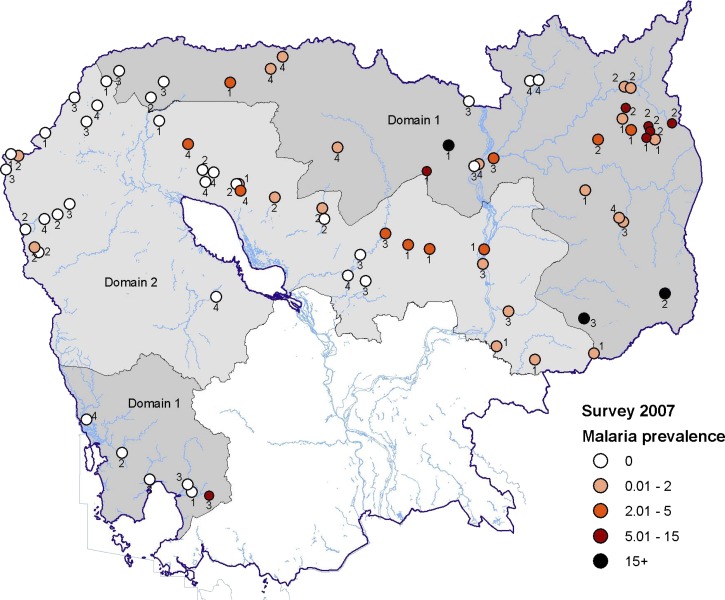
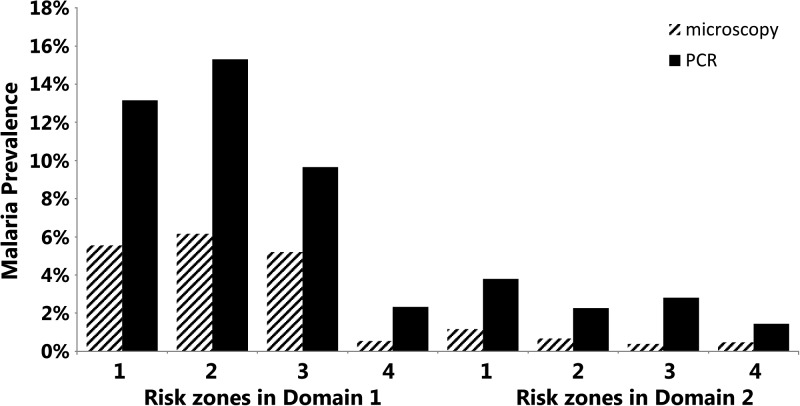
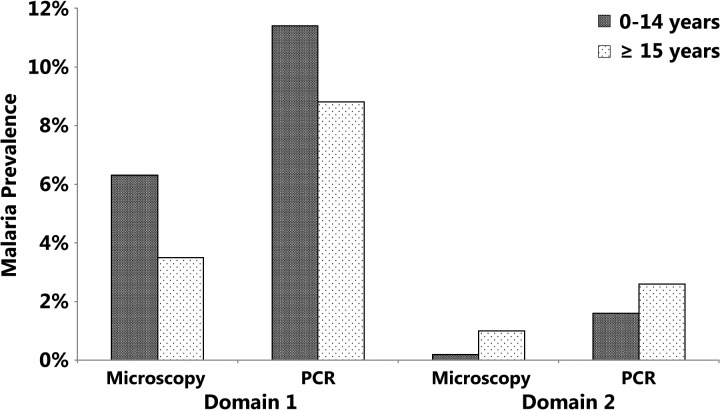
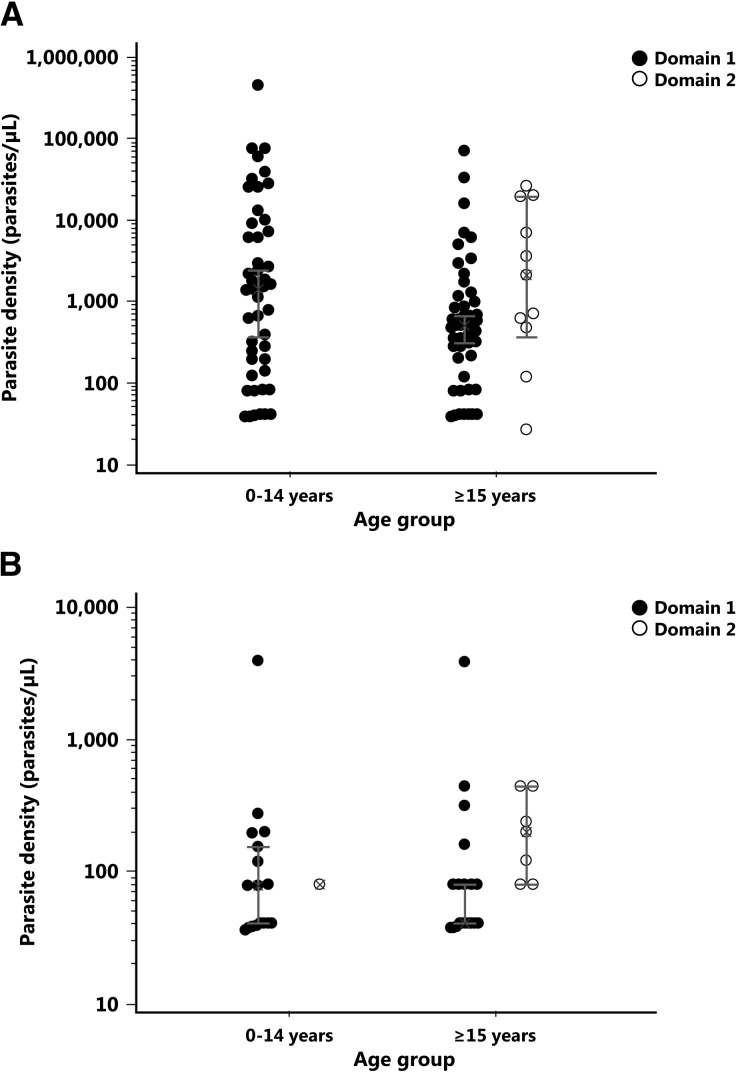
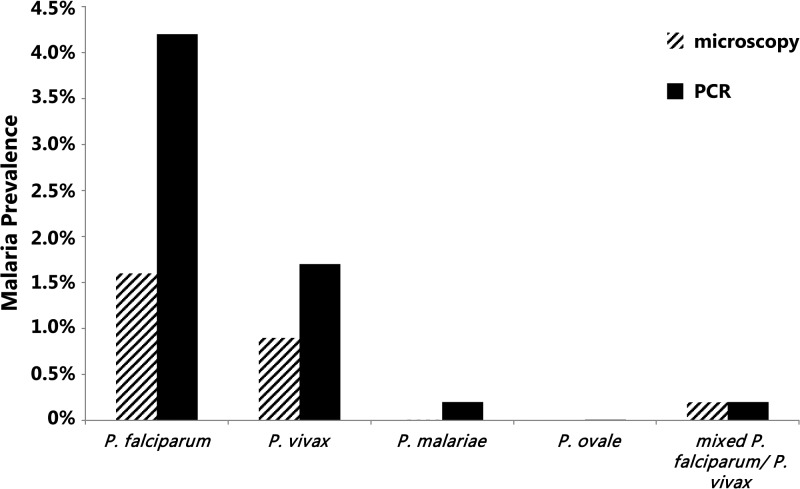
Accurate information regarding malaria prevalence at national level is required to design and assess malaria control/elimination efforts. Although many comparisons of microscopy and polymerase chain reaction (PCR)-based methods have been conducted, there is little published literature covering such comparisons in southeast Asia especially at the national level. Both microscopic examination and PCR detection were performed on blood films and dried blood spots samples collected from 8,067 individuals enrolled in a nationwide, stratified, multistage, cluster sampling malaria prevalence survey conducted in Cambodia in 2007. The overall malaria prevalence and prevalence rates of Plasmodium falciparum, Plasmodium vivax, and Plasmodium malariae infections estimated by microscopy (N = 8,067) were 2.74% (95% confidence interval [CI]: 2.39-3.12%), 1.81% (95% CI: 1.53-2.13%), 1.14% (95% CI: 0.92-1.40%), and 0.01% (95% CI: 0.003-0.07%), respectively. The overall malaria prevalence based on PCR detection (N = 7,718) was almost 2.5-fold higher (6.31%, 95% CI: 5.76-6.89%, P < 0.00001). This difference was significantly more pronounced for P. falciparum (4.40%, 95% CI: 3.95-4.90%, P < 0.00001) compared with P. vivax (1.89%, 95% CI: 1.60-2.22%, P < 0.001) and P. malariae infections (0.22%, 95% CI: 0.13-0.35%, P < 0.0001). The significant proportion of microscopy-negative but PCR-positive individuals (289/7,491, 3.85%) suggest microscopic examination frequently underestimated malaria infections and that active case detection based on microscopy may miss a significant reservoir of infection, especially in low-transmission settings.
© The American Society of Tropical Medicine and Hygiene.
Figures
Similar articles
-
Forest malaria in Cambodia: the occupational and spatial clustering of Plasmodium vivax and Plasmodium falciparum infection risk in a cross-sectional survey in Mondulkiri province, Cambodia.Malar J. 2020 Nov 19;19(1):413. doi: 10.1186/s12936-020-03482-4. Malar J. 2020. PMID: 33213471 Free PMC article.
-
A large proportion of asymptomatic Plasmodium infections with low and sub-microscopic parasite densities in the low transmission setting of Temotu Province, Solomon Islands: challenges for malaria diagnostics in an elimination setting.Malar J. 2010 Sep 7;9:254. doi: 10.1186/1475-2875-9-254. Malar J. 2010. PMID: 20822506 Free PMC article.
-
Microscopic and molecular evidence of the presence of asymptomatic Plasmodium falciparum and Plasmodium vivax infections in an area with low, seasonal and unstable malaria transmission in Ethiopia.BMC Infect Dis. 2015 Aug 5;15:310. doi: 10.1186/s12879-015-1070-1. BMC Infect Dis. 2015. PMID: 26242405 Free PMC article.
-
Submicroscopic Plasmodium prevalence in relation to malaria incidence in 20 villages in western Cambodia.Malar J. 2017 Jan 31;16(1):56. doi: 10.1186/s12936-017-1703-5. Malar J. 2017. PMID: 28143518 Free PMC article.
-
Detection of mixed infection level of Plasmodium falciparum and Plasmodium vivax by SYBR Green I-based real-time PCR in North Gondar, north-west Ethiopia.Malar J. 2014 Oct 18;13:411. doi: 10.1186/1475-2875-13-411. Malar J. 2014. PMID: 25326079 Free PMC article.
Cited by
-
Challenges in Laboratory Diagnosis of Malaria in a Low-Resource Country at Tertiary Care in Eastern Nepal: A Comparative Study of Conventional vs. Molecular Methodologies.J Trop Med. 2021 Dec 28;2021:3811318. doi: 10.1155/2021/3811318. eCollection 2021. J Trop Med. 2021. PMID: 34992661 Free PMC article.
-
The primate malaria parasites Plasmodium malariae, Plasmodium brasilianum and Plasmodium ovale spp.: genomic insights into distribution, dispersal and host transitions.Malar J. 2022 May 3;21(1):138. doi: 10.1186/s12936-022-04151-4. Malar J. 2022. PMID: 35505317 Free PMC article. Review.
-
Contribution of real-time PCR to Plasmodium species identification and to clinical decisions: a nationwide study in a non-endemic setting.Eur J Clin Microbiol Infect Dis. 2017 Apr;36(4):671-675. doi: 10.1007/s10096-016-2844-0. Epub 2016 Dec 13. Eur J Clin Microbiol Infect Dis. 2017. PMID: 27966198
-
Forest malaria in Cambodia: the occupational and spatial clustering of Plasmodium vivax and Plasmodium falciparum infection risk in a cross-sectional survey in Mondulkiri province, Cambodia.Malar J. 2020 Nov 19;19(1):413. doi: 10.1186/s12936-020-03482-4. Malar J. 2020. PMID: 33213471 Free PMC article.
-
Insecticide-treated nets and malaria prevalence, Papua New Guinea, 2008-2014.Bull World Health Organ. 2017 Oct 1;95(10):695-705B. doi: 10.2471/BLT.16.189902. Epub 2017 Sep 5. Bull World Health Organ. 2017. PMID: 29147042 Free PMC article.
References
-
- Ariey F, Witkowski B, Amaratunga C, Beghain J, Langlois AC, Khim N, Kim S, Duru V, Bouchier C, Ma L, Lim P, Leang R, Duong S, Sreng S, Suon S, Chuor CM, Bout DM, Menard S, Rogers WO, Genton B, Fandeur T, Miotto O, Ringwald P, Le Bras J, Berry A, Barale JC, Fairhurst RM, Benoit-Vical F, Mercereau-Puijalon O, Menard D. A molecular marker of artemisinin-resistant Plasmodium falciparum malaria. Nature. 2014;505:50–55. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
