

Effect of chorionic villus sampling on the occurrence of preeclampsia and gestational hypertension: An updated systematic review and meta-analysis
- PMID: 27403071
- PMCID: PMC4922727
- DOI: 10.5152/jtgga.2016.16026
Effect of chorionic villus sampling on the occurrence of preeclampsia and gestational hypertension: An updated systematic review and meta-analysis
Abstract
Objective: To perform a meta-analysis for an assessment of the risk of preeclampsia or gestational hypertension following chorionic villus sampling (CVS).
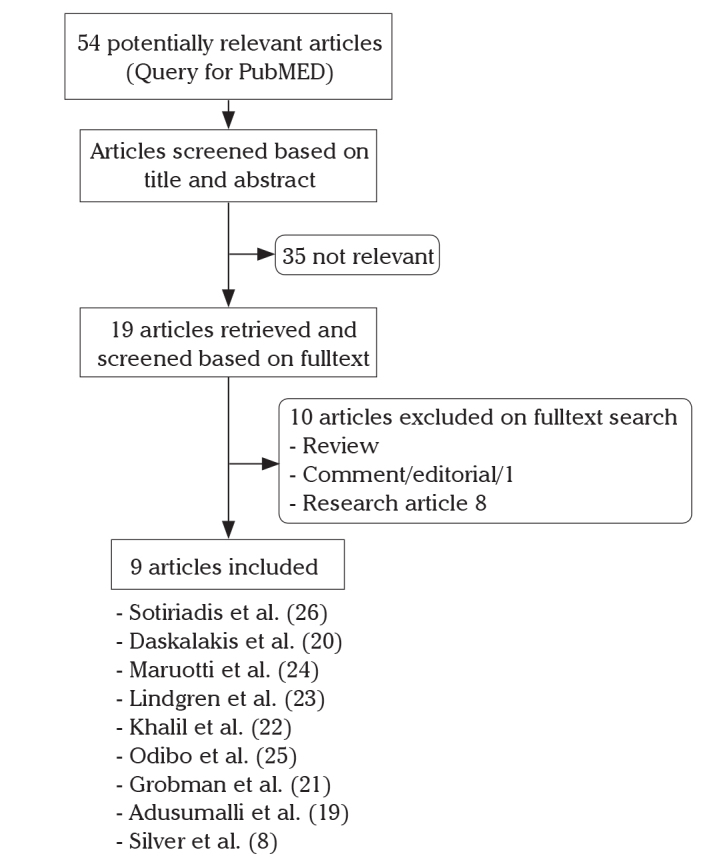
Data source: PubMed was systematically searched from its inception through January 2016.
Material and methods: Nine reports were identified. A pre-specified scale was used to assess their quality.
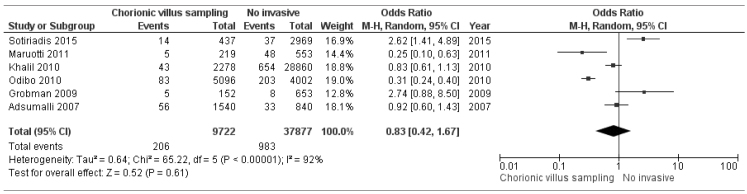
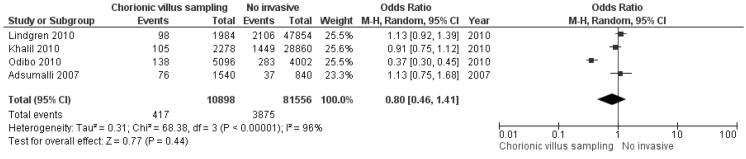
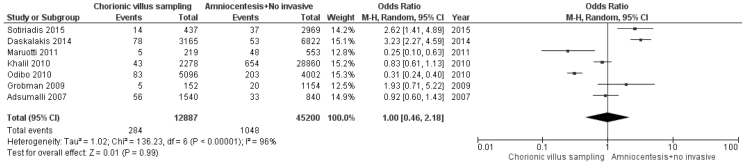
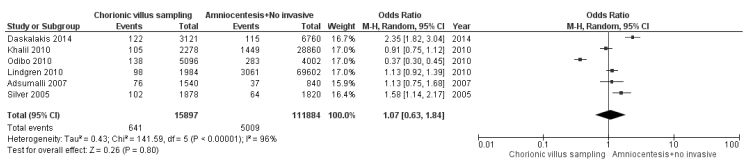
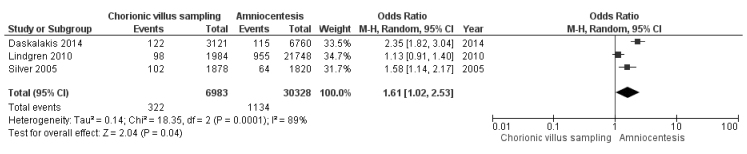
Tabulation integration and results: We performed pooling into three subgroups with respect to the control group: A) Patients with no invasive prenatal diagnostic procedure served as a control group for comparison. The odds ratios for gestational hypertension (0.76, 95% CI 0.46-1.26), preeclampsia (0.83, 95% CI 0.42-1.67), and severe preeclampsia (0.49, 95% CI 0.04-5.78) or when hypertension categories were pooled (0.80, 95% CI 0.46-1.41) were not significantly different. B) Patients with midtrimester diagnostic amniocentesis and patients with no invasive prenatal diagnostic procedure were combined as a control group for comparison. The odds ratios for preeclampsia (1, 95% CI 0.46-2.18), severe preeclampsia (0.83, 95% CI 0.14-4.85), and pooled hypertension categories (1.07, 95% CI 0.63-1.84) were not significantly different. C) Patients with midtrimester diagnostic amniocentesis served as a control group. There was a significant difference in the odds ratio for preeclampsia between the CVS and amniocentesis groups (2.47, 95% CI 1.14-5.33). There was a marginal difference in the odds ratio for combined pregnancy-induced hypertension categories between the CVS and amniocentesis groups (1.61, 95% CI 1.02-2.53).
Conclusion: The available data do not indicate an increased risk of preeclampsia or gestational hypertension following first trimester CVS. The heterogeneity and retrospective design of existing studies are limiting factors for our analysis and findings.
Keywords: Meta-analysis; chorionic villus sampling; midtrimester diagnostic amniocentesis; preeclampsia.
Figures




References
-
- Duley L. Maternal mortality associated with hypertensive disorders of pregnancy in Africa, Asia, Latin America and the Caribbean. Br J Obstet Gynaecol. 1992;99:547–53. http://dx.doi.org/10.1111/j.1471-0528.1992.tb13818.x. - DOI - PubMed
-
- Gupta S, Agarwal A, Sharma RK. The role of placental oxidative stress and lipid peroxidation in preeclampsia. Obstet Gynecol Surv. 2005;60:807–16. http://dx.doi.org/10.1097/01.ogx.0000193879.79268.59. - DOI - PubMed
-
- Redman CW. Preeclampsia: a multi-stress disorder. Rev Med Interne. 2011;32(Suppl 1):S41–4. http://dx.doi.org/10.1016/j.revmed.2011.03.331. - DOI - PubMed
-
- Carty DM, Delles C, Dominiczak AF. Preeclampsia and future maternal health. J Hypertens. 2010;28:1349–55. http://dx.doi.org/10.1097/HJH.0b013e32833a39d0. - DOI - PubMed
-
- Lyall F. Mechanisms regulating cytotrophoblast invasion in normal pregnancy and pre-eclampsia. Aust N Z J Obstet Gynaecol. 2006;46:266–73. http://dx.doi.org/10.1111/j.1479-828X.2006.00589.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources