

Comparison of AIMS65, Glasgow-Blatchford score, and Rockall score in a European series of patients with upper gastrointestinal bleeding: performance when predicting in-hospital and delayed mortality
- PMID: 27403303
- PMCID: PMC4924428
- DOI: 10.1177/2050640615604779
Comparison of AIMS65, Glasgow-Blatchford score, and Rockall score in a European series of patients with upper gastrointestinal bleeding: performance when predicting in-hospital and delayed mortality
Abstract
Objective: AIMS65 is a score designed to predict in-hospital mortality, length of stay, and costs of gastrointestinal bleeding. Our aims were to revalidate AIMS65 as predictor of inpatient mortality and to compare AIMS65's performance with that of Glasgow-Blatchford (GBS) and Rockall scores (RS) with regard to mortality, and the secondary outcomes of a composite endpoint of severity, transfusion requirements, rebleeding, delayed (6-month) mortality, and length of stay.
Methods: The study included 309 patients. Clinical and biochemical data, transfusion requirements, endoscopic, surgical, or radiological treatments, and outcomes for 6 months after admission were collected. Clinical outcomes were in-hospital mortality, delayed mortality, rebleeding, composite endpoint, blood transfusions, and length of stay.
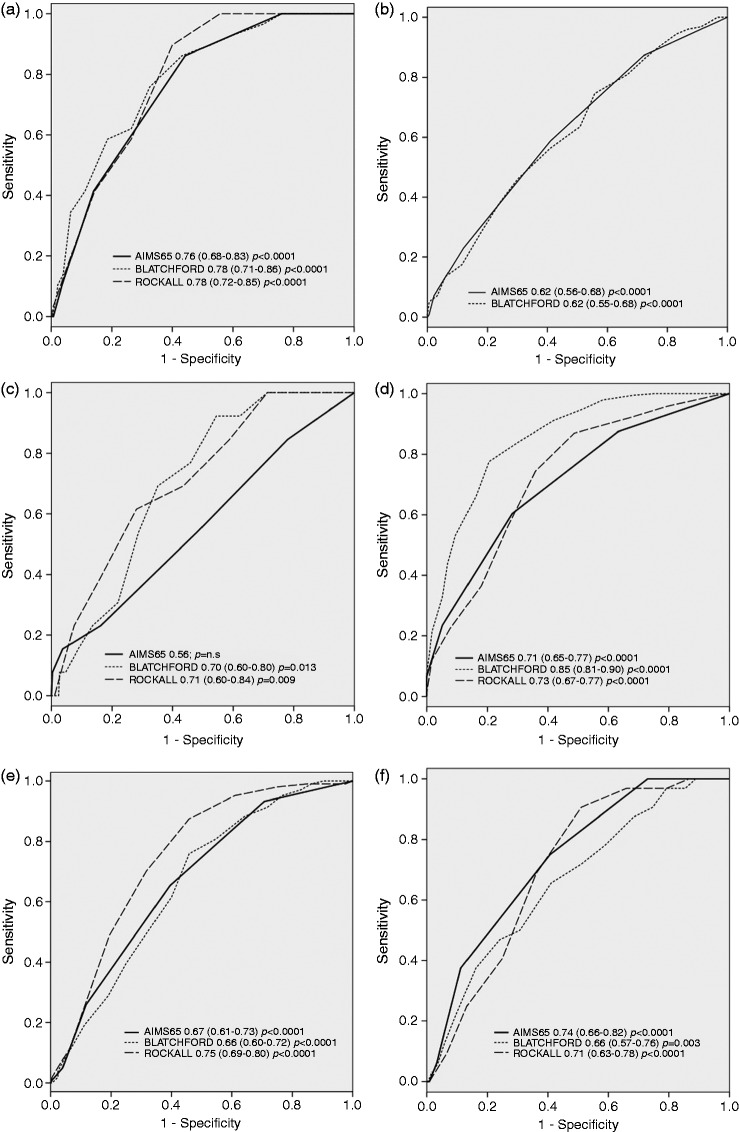
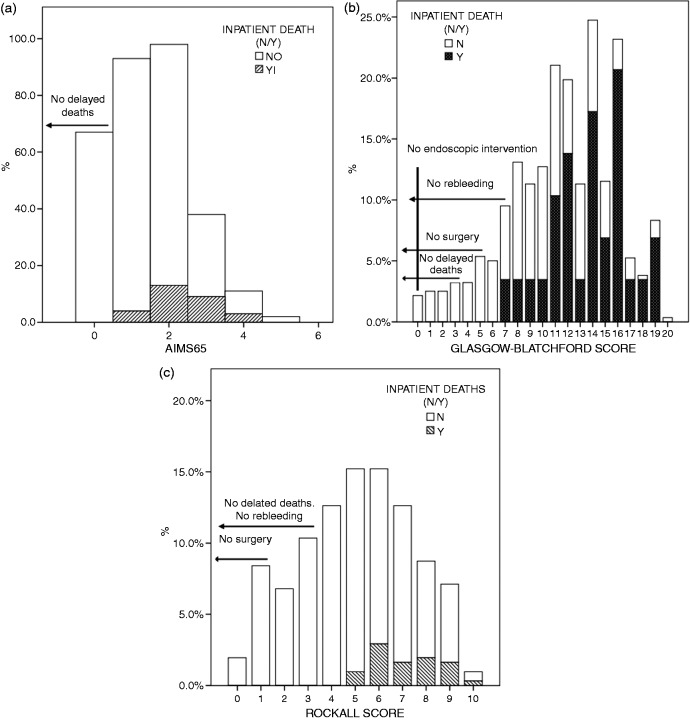
Results: In receiver-operating characteristic curve analyses, AIMS65, GBS, and RS were similar when predicting inpatient mortality (0.76 vs. 0.78 vs. 0.78). Regarding endoscopic intervention, AIMS65 and GBS were identical (0.62 vs. 0.62). AIMS65 was useless when predicting rebleeding compared to GBS or RS (0.56 vs. 0.70 vs. 0.71). GBS was better at predicting the need for transfusions. No patient with AIMS65 = 0, GBS ≤ 6, or RS ≤ 4 died. Considering the composite endpoint, an AIMS65 of 0 did not exclude high risk patients, but a GBS ≤ 1 or RS ≤ 2 did. The three scores were similar in predicting prolonged in-hospital stay. Delayed mortality was better predicted by AIMS65.
Conclusion: AIMS65 is comparable to GBS and RS in essential endpoints such as inpatient mortality, the need for endoscopic intervention and length of stay. GBS is a better score predicting rebleeding and the need for transfusion, but AIMS65 shows a better performance predicting delayed mortality.
Keywords: AIMS65; Glasgow–Blatchford score; Rockall score; Upper gastrointestinal bleeding.
Figures
Similar articles
-
Risk stratification in acute upper GI bleeding: comparison of the AIMS65 score with the Glasgow-Blatchford and Rockall scoring systems.Gastrointest Endosc. 2016 Jun;83(6):1151-60. doi: 10.1016/j.gie.2015.10.021. Epub 2015 Oct 26. Gastrointest Endosc. 2016. PMID: 26515955
-
Comparison of risk scoring systems for patients presenting with upper gastrointestinal bleeding: international multicentre prospective study.BMJ. 2017 Jan 4;356:i6432. doi: 10.1136/bmj.i6432. BMJ. 2017. PMID: 28053181 Free PMC article.
-
Comparison of three risk scores to predict outcomes in upper gastrointestinal bleeding; modifying Glasgow-Blatchford with albumin.Rom J Intern Med. 2019 Dec 1;57(4):322-333. doi: 10.2478/rjim-2019-0016. Rom J Intern Med. 2019. PMID: 31268861
-
Comparative diagnostic utility of Rockall and Glasgow-Blatchford scores in non-variceal upper gastrointestinal bleeding: a systematic review and meta-analysis.Eur J Gastroenterol Hepatol. 2025 Feb 1;37(2):161-166. doi: 10.1097/MEG.0000000000002867. Epub 2024 Dec 18. Eur J Gastroenterol Hepatol. 2025. PMID: 39400553
-
Pre-Endoscopic Scores Predicting Low-Risk Patients with Upper Gastrointestinal Bleeding: A Systematic Review and Meta-Analysis.J Clin Med. 2023 Aug 9;12(16):5194. doi: 10.3390/jcm12165194. J Clin Med. 2023. PMID: 37629235 Free PMC article. Review.
Cited by
-
Management of non-variceal upper gastrointestinal bleeding: where are we in 2018?Frontline Gastroenterol. 2019 Jan;10(1):35-42. doi: 10.1136/flgastro-2017-100901. Epub 2018 Feb 9. Frontline Gastroenterol. 2019. PMID: 30651955 Free PMC article. Review.
-
Prediction of adverse outcomes using non-endoscopic scoring systems in patients over 80 years of age who present with the upper gastrointestinal bleeding in the emergency department.Ulus Travma Acil Cerrahi Derg. 2022 Jan;28(1):39-47. doi: 10.14744/tjtes.2020.27810. Ulus Travma Acil Cerrahi Derg. 2022. PMID: 34967427 Free PMC article.
-
A Nomogram Model for Prediction of Mortality Risk of Patients with Dangerous Upper Gastrointestinal Bleeding: A Two-center Retrospective Study.Curr Med Sci. 2023 Aug;43(4):723-732. doi: 10.1007/s11596-023-2748-z. Epub 2023 Jun 16. Curr Med Sci. 2023. PMID: 37326886
-
Comparison of Glasgow-Blatchford score and full Rockall score systems to predict clinical outcomes in patients with upper gastrointestinal bleeding.Clin Exp Gastroenterol. 2016 Oct 31;9:337-343. doi: 10.2147/CEG.S114860. eCollection 2016. Clin Exp Gastroenterol. 2016. PMID: 27826205 Free PMC article.
-
An update on the management of non-variceal upper gastrointestinal bleeding.Gastroenterol Rep (Oxf). 2023 Mar 20;11:goad011. doi: 10.1093/gastro/goad011. eCollection 2023. Gastroenterol Rep (Oxf). 2023. PMID: 36949934 Free PMC article. Review.
References
-
- Hearnshaw SA, Logan RF, Lowe D, et al. Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut 2011; 60: 1327–1335. - PubMed
-
- Van Leerdam ME, Vreeburg EM, Rauws EA, et al. Acute upper GI bleeding: did anything change? Time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000. Am J Gastroenterol 2003; 98: 1494–1499. - PubMed
-
- Barkun A, Sabbah S, Enns R, et al. The Canadian Registry on Nonvariceal Upper Gastrointestinal Bleeding and Endoscopy (RUGBE): endoscopic hemostasis and proton pump inhibition are associated with improved outcomes in a real-life setting. Am J Gastroenterol 2004; 99: 1238–1246. - PubMed
-
- Jairath V, Kahan BC, Logan RF, et al. Outcomes following acute nonvariceal upper gastrointestinal bleeding in relation to time to endoscopy: results from a nationwide study. Endoscopy 2012; 44: 723–730. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
