

Knife-assisted snare resection (KAR) of large and refractory colonic polyps at a Western centre: Feasibility, safety and efficacy study to guide future practice
- PMID: 27403314
- PMCID: PMC4924438
- DOI: 10.1177/2050640615615301
Knife-assisted snare resection (KAR) of large and refractory colonic polyps at a Western centre: Feasibility, safety and efficacy study to guide future practice
Abstract
Objective: Endoscopic mucosal resection (EMR) is widely practiced in western countries. Endoscopic submucosal dissection (ESD) is very effective for treating complex polyps but colonic ESD in the western setting remains challenging. We have developed a novel technique of knife-assisted snare resection (KAR) for the resection of these complex lesions. Here we aim to describe the technique, evaluate its outcomes, identify outcome predictors and define its learning curve.
Methods: We conducted a prospective cohort study of patients who had large and refractory polyps resected by KAR at our institution from 2007 to 2013. Polyp characteristics and procedure details were recorded. Endoscopic follow-up was performed to identify recurrence.
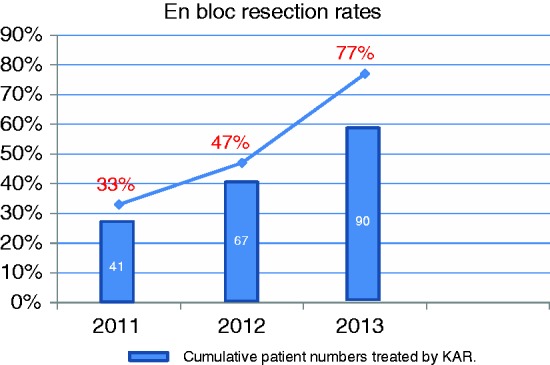
Results: A total of 170 patients with polyps 20-170 mm in size were treated by KAR and followed up for a mean of 31.5 months (range 12-84 months). 29% of the polyps were >50 mm, 22% had fibrosis from previous unsuccessful interventions and 25% were in the right colon. The perforation rate (1.2%) and bleeding rate (4.7%) were acceptable and managed conservatively in most patients. Recurrence rate after the first attempt was 13.1%. Recurrence was significantly increased by polyp size >50 mm (p = 0.008; OR 5.03, 95% CI 1.54-16.48), presence of fibrosis (p = 0.002; OR 6.59, 95% CI 1.97-22.07) and piecemeal resection (p < 0.001; OR 0.31, CI 0.078-1.12). Cure rates were 87% after the first attempt, improving to 95.6% with further attempts. En bloc resection rate showed a linear increase and reached almost 80% as the endoscopist's cumulative experience approached 100 cases.
Conclusion: This is the largest reported Western series on KAR in the colon. We have demonstrated the feasibility, efficacy and safety of this technique in the treatment of complex polyps, with or without fibrosis and at all sites. KAR has shown better outcomes than either EMR or ESD. We have also managed to identify significant outcome predictors and define the learning curve.
Keywords: EMR; ESD; Endoscopic mucosal resection; colonic polyps; colonoscopy; difficult polyps; endoscopic submucosal dissection.
Figures
Similar articles
-
Multicenter evaluation of recurrence in endoscopic submucosal dissection and endoscopic mucosal resection in the colon: A Western perspective.World J Gastrointest Endosc. 2023 Jun 16;15(6):458-468. doi: 10.4253/wjge.v15.i6.458. World J Gastrointest Endosc. 2023. PMID: 37397977 Free PMC article.
-
Knife-assisted snare resection: a novel technique for resection of scarred polyps in the colon.Endoscopy. 2016 Mar;48(3):277-80. doi: 10.1055/s-0035-1569647. Epub 2016 Jan 28. Endoscopy. 2016. PMID: 26820175 Clinical Trial.
-
Beyond the snare: technically accessible large en bloc colonic resection in the West: an animal study.Dig Endosc. 2012 Jan;24(1):21-9. doi: 10.1111/j.1443-1661.2011.01154.x. Epub 2011 Apr 18. Dig Endosc. 2012. PMID: 22211408
-
Endoscopic Mucosal Resection and Endoscopic Submucosal Dissection.Clin Colon Rectal Surg. 2023 Aug 7;37(5):277-288. doi: 10.1055/s-0043-1770941. eCollection 2024 Sep. Clin Colon Rectal Surg. 2023. PMID: 39132198 Free PMC article. Review.
-
Endoscopic mucosal resection and endoscopic submucosal dissection of large colonic polyps.Nat Rev Gastroenterol Hepatol. 2016 Aug;13(8):486-96. doi: 10.1038/nrgastro.2016.96. Epub 2016 Jun 29. Nat Rev Gastroenterol Hepatol. 2016. PMID: 27353401 Review.
Cited by
-
Hybrid endoscopic submucosal dissection: An alternative resection modality for large laterally spreading tumors in the cecum?BMC Gastroenterol. 2021 May 5;21(1):203. doi: 10.1186/s12876-021-01766-w. BMC Gastroenterol. 2021. PMID: 33952206 Free PMC article.
-
Polypectomy and advanced endoscopic resection.Frontline Gastroenterol. 2017 Apr;8(2):110-114. doi: 10.1136/flgastro-2016-100769. Epub 2017 Feb 10. Frontline Gastroenterol. 2017. PMID: 28839894 Free PMC article. Review.
-
Modified endoscopic mucosal resection techniques for treating precancerous colorectal lesions.Ann Gastroenterol. 2021 Nov-Dec;34(6):757-769. doi: 10.20524/aog.2021.0647. Epub 2021 Jul 2. Ann Gastroenterol. 2021. PMID: 34815641 Free PMC article. Review.
-
Current Endoscopic Resection Techniques for Gastrointestinal Lesions: Endoscopic Mucosal Resection, Submucosal Dissection, and Full-Thickness Resection.Visc Med. 2021 Oct;37(5):358-371. doi: 10.1159/000515354. Epub 2021 Mar 31. Visc Med. 2021. PMID: 34722719 Free PMC article. Review.
-
Endoscopic Submucosal Dissection (ESD) for the Management of Fibrotic Non-Lifting Colorectal Lesions (NLCLs): Results from a Large Multicenter Retrospective Study.Cancers (Basel). 2025 Apr 6;17(7):1242. doi: 10.3390/cancers17071242. Cancers (Basel). 2025. PMID: 40227777 Free PMC article.
References
-
- Swan MP, Bourke MJ, Alexander S, et al. Large refractory colonic polyps: Is it time to change our practice? A prospective study of the clinical and economic impact of a tertiary referral colonic mucosal resection and polypectomy service (with videos). Gastrointest Endosc 2009; 70: 1128–1136. - PubMed
-
- Khasab M, Eid E, Rusche M, et al. Incidence and predictors of “late” recurrences after endoscopic piecemeal resection of large sessile adenomas. Gastrointest Endosc 2009; 70: 344–349. - PubMed
-
- Kedia P, Waye JD. Colon polypectomy: A review of routine and advanced techniques. J Clin Gastroenterol 2013; 47: 657–665. - PubMed
-
- Niimi K, Fujishiro M, Kodashima S, et al. Long-term outcomes of endoscopic submucosal dissection for colorectal epithelial neoplasms. Endoscopy 2010; 42: 723–729. - PubMed
-
- Toyonaga T, Man-i M, Fujita T, et al. Retrospective study of technical aspects and complications of endoscopic submucosal dissection for laterally spreading tumors of the colorectum. Endoscopy 2010; 42: 714–722. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
