

Arteriovenous Fistula Embolization in Suspected Parauterine Choriocarcinoma
- PMID: 27403360
- PMCID: PMC4923520
- DOI: 10.1155/2016/6353471
Arteriovenous Fistula Embolization in Suspected Parauterine Choriocarcinoma
Abstract
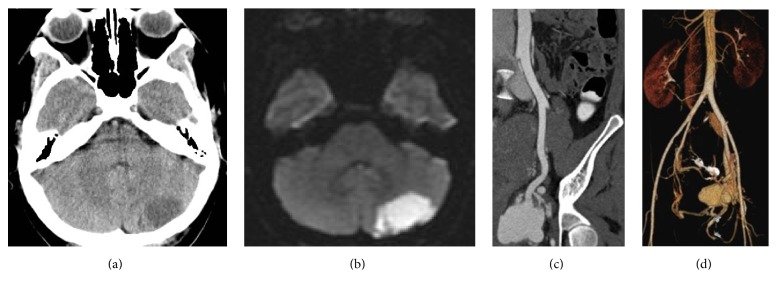
This is a case of choriocarcinoma that did not regress after chemotherapy treatment. A 30-year-old female patient (gravida 2, para 2), presented to our ER with stroke and persistent mild pelvic pain 2 months after a Caesarean section. Computed tomography (CT) revealed an ischemic left hemicerebellar region and a hypervascular mass in the pelvic region. This mass was not present on routine fetal ultrasound during pregnancy. The lesion was treated by chemotherapy after closure of a foramen ovale and insertion of an inferior vena cava (IVC) filter. After that, 2 courses of EMACO (Etoposide, Methotrexate, Actinomycin D, Cyclophosphamide, and Vincristine) chemotherapy regimen were given. Posttreatment CT showed the hypervascular mass without any changes. Arteriography showed the arteriovenous fistulae that were embolized successfully with plugs, coils, and glue. Embolization was considered due to the risk of acute hemorrhagic life-threatening complications. Eight chemotherapy courses were added after embolization. Treatment by endovascular approach and reduction of the hypervascular mass can be a valuable adjunct to chemotherapy treatment of choriocarcinoma.
Figures



References
-
- Lurain J. R. Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. American Journal of Obstetrics and Gynecology. 2010;203(6):531–539. doi: 10.1016/j.ajog.2010.06.073. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
