High Prevalence of Liver Fibrosis in Patients with Human Immunodeficiency Virus Monoinfection and Human Immunodeficiency Virus Hepatitis-B Co-infection as Assessed by Shear Wave Elastography: Study at a Teaching Hospital in Kenya
- PMID: 27403400
- PMCID: PMC4926547
- DOI: 10.4103/2156-7514.183582
High Prevalence of Liver Fibrosis in Patients with Human Immunodeficiency Virus Monoinfection and Human Immunodeficiency Virus Hepatitis-B Co-infection as Assessed by Shear Wave Elastography: Study at a Teaching Hospital in Kenya
Abstract
Objectives: The aim of this study was to determine the prevalence of liver fibrosis in patients with human immunodeficiency virus (HIV) monoinfection versus those with HIV hepatitis-B virus (HBV) co-infection as assessed with shear wave elastography (SWE) in a tertiary sub-Saharan Africa hospital.
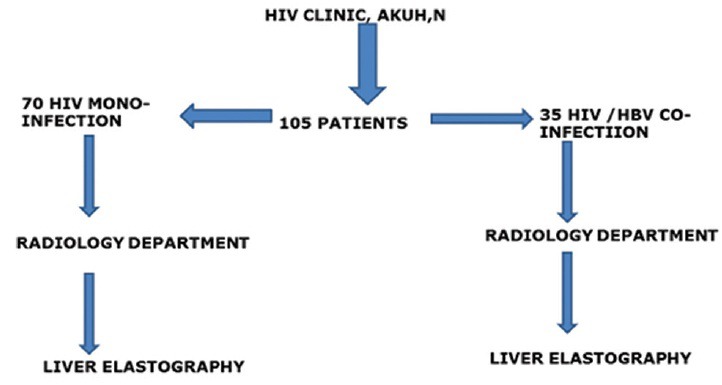
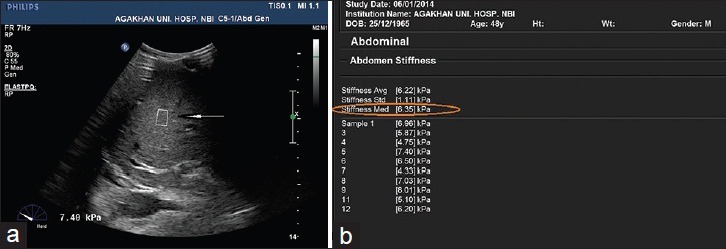
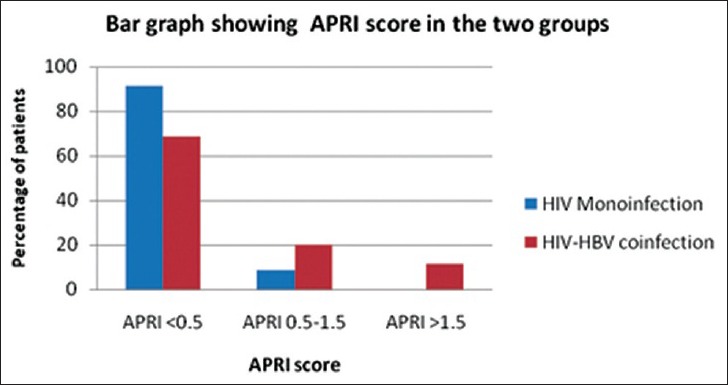
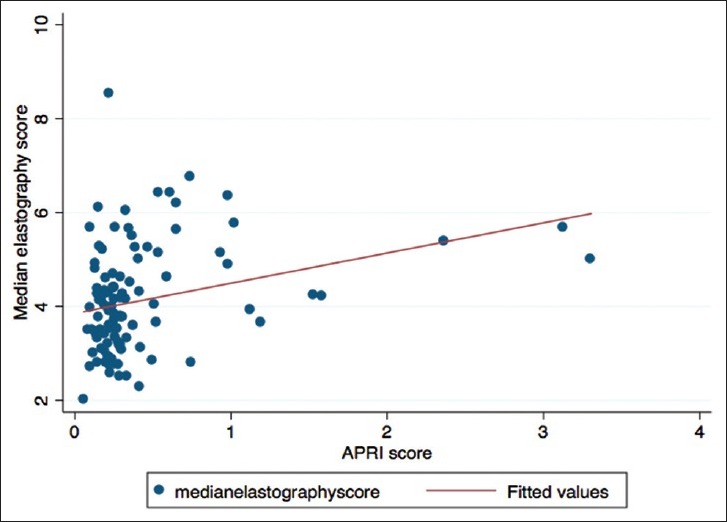
Materials and methods: A total of 105 consecutive patients, 70 with HIV monoinfection and 35 with HIV-HBV co-infection, had liver elastography obtained using SWE to assess for the presence of liver fibrosis the cutoff of which was 5.6 kPa. Assessment of aspartate aminotransferase-to-platelet ratio index (APRI) score (a noninvasive serum biomarker of liver fibrosis) in these patients was also done.
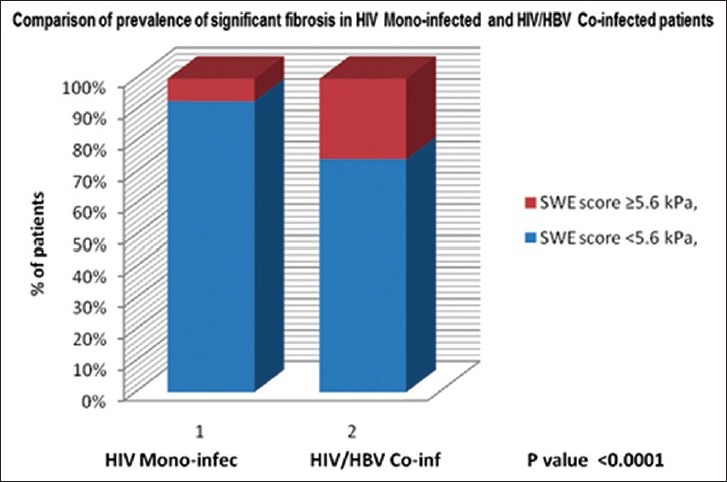
Results: The prevalence of liver fibrosis was significantly higher (P < 0.0001) in patients with HIV-HBV co-infection, 25.7%, compared to those with HIV monoinfection, 7.1%. APRI score was greater in patients with HIV-HBV co-infection than those with HIV monoinfection. HIV co-infection with HBV accelerates progression to liver fibrosis. Association of a low cluster of differentiation 4 (CD-4) count with advanced fibrosis supports earlier starting of antiretroviral therapy to prevent rapid progression of liver disease in HIV-positive patients.
Conclusion: In view of the high prevalence of liver fibrosis in patients with HIV-HBV co-infection, regular monitoring of the disease progression is recommended.
Keywords: Hepatitis-B; Human immunodeficiency virus; liver fibrosis; shear wave elastography.
Figures

References
-
- Smith C, Sabin CA, Lundgren JD, Thiebaut R, Weber R, et al. Data Collection on Adverse Events of Anti-HIV drugs (D: A: D) Study Group. Factors associated with specific causes of death amongst HIV-positive individuals in the D: A: D Study. AIDS. 2010;24:1537–48. - PubMed
-
- Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol. 2006;44(1 Suppl):S6–9. - PubMed
-
- Wai CT, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA, Conjeevaram HS, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38:518–26. - PubMed
-
- Lin ZH, Xin YN, Dong QJ, Wang Q, Jiang XJ, Zhan SH, et al. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology. 2011;53:726–36. - PubMed
-
- Duarte-Rojo A, Altamirano JT, Feld JJ. Noninvasive markers of fibrosis: Key concepts for improving accuracy in daily clinical practice. Ann Hepatol. 2012;11:426–39. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials