Fungal Infections of the Central Nervous System: A Pictorial Review
- PMID: 27403402
- PMCID: PMC4926551
- DOI: 10.4103/2156-7514.184244
Fungal Infections of the Central Nervous System: A Pictorial Review
Abstract
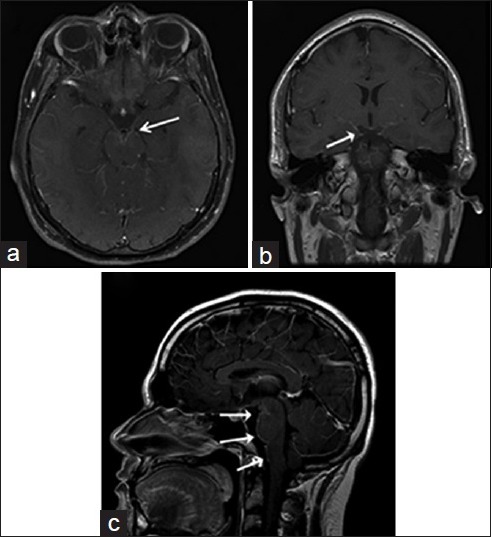
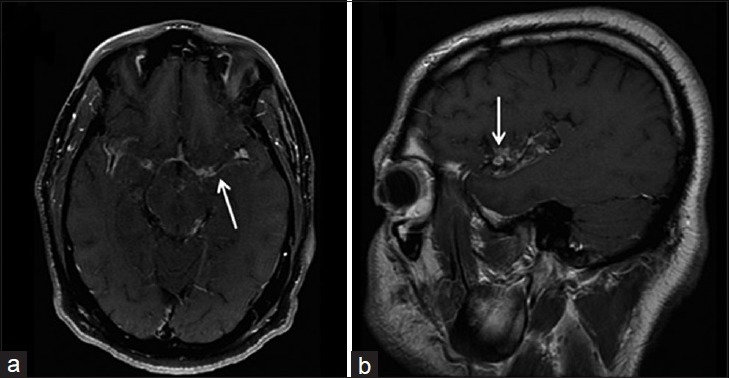
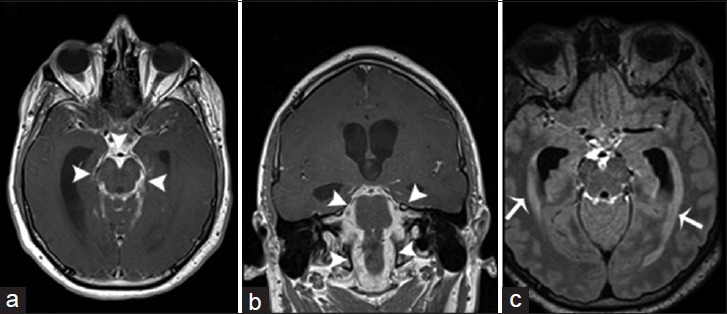
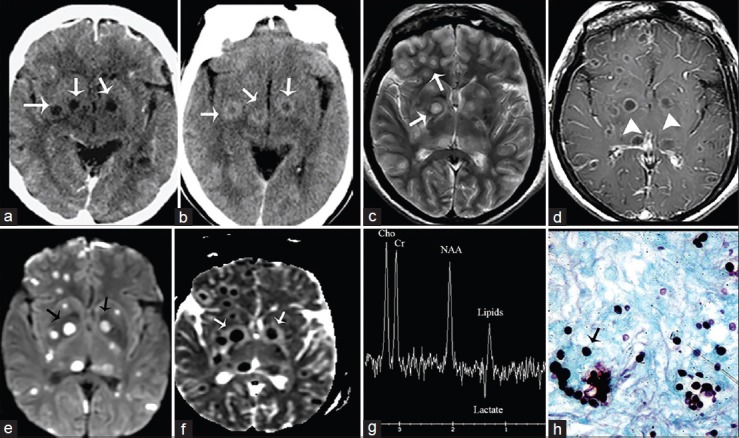
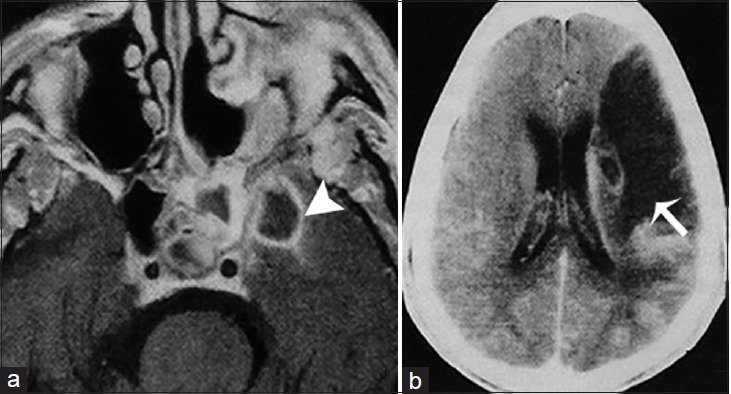
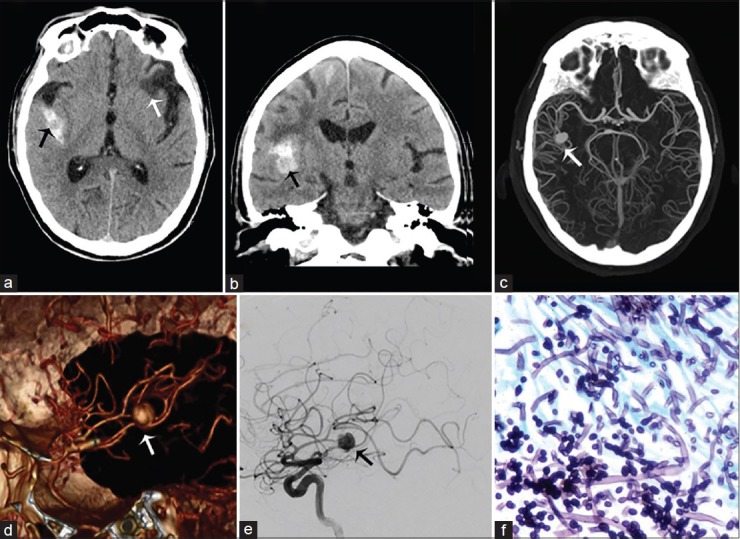
Fungal infections of the central nervous system (CNS) pose a threat to especially immunocompromised patients and their development is primarily determined by the immune status of the host. With an increasing number of organ transplants, chemotherapy, and human immunodeficiency virus infections, the number of immunocompromised patients as susceptible hosts is growing and fungal infections of the CNS are more frequently encountered. They may result in meningitis, cerebritis, abscess formation, cryptococcoma, and meningeal vasculitis with rapid disease progression and often overlapping symptoms. Although radiological characteristics are often nonspecific, unique imaging patterns can be identified through computer tomography as a first imaging modality and further refined by magnetic resonance imaging. A rapid diagnosis and the institution of the appropriate therapy are crucial in helping prevent an often fatal outcome.
Keywords: Brain abscess; cryptococcoma; fungal cerebritis; fungal meningitis; human immune deficiency virus; vascular cerebral fungal infections.
Figures

References
-
- Mohan S, Jain KK, Arabi M, Shah GV. Imaging of meningitis and ventriculitis. Neuroimaging Clin N Am. 2012;22:557–83. - PubMed
-
- Mathur M, Johnson CE, Sze G. Fungal infections of the central nervous system. Neuroimaging Clin N Am. 2012;22:609–32. - PubMed
-
- Aiken AH. Central nervous system infection. Neuroimaging Clin N Am. 2010;20:557–80. - PubMed
-
- Jain KK, Mittal SK, Kumar S, Gupta RK. Imaging features of central nervous system fungal infections. Neurol India. 2007;55:241–50. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources