

Cerebral blood flow and autoregulation: current measurement techniques and prospects for noninvasive optical methods
- PMID: 27403447
- PMCID: PMC4914489
- DOI: 10.1117/1.NPh.3.3.031411
Cerebral blood flow and autoregulation: current measurement techniques and prospects for noninvasive optical methods
Abstract
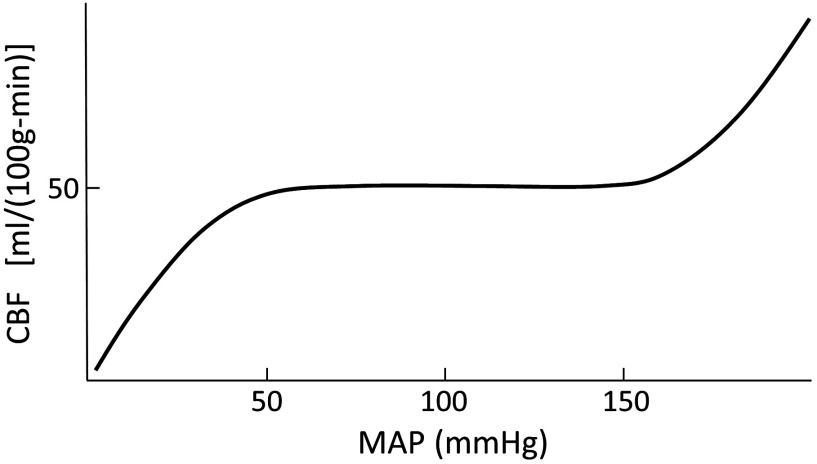
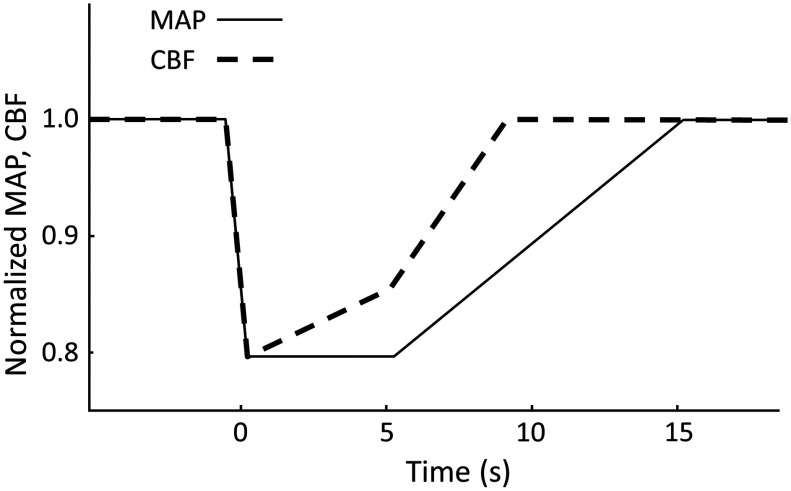
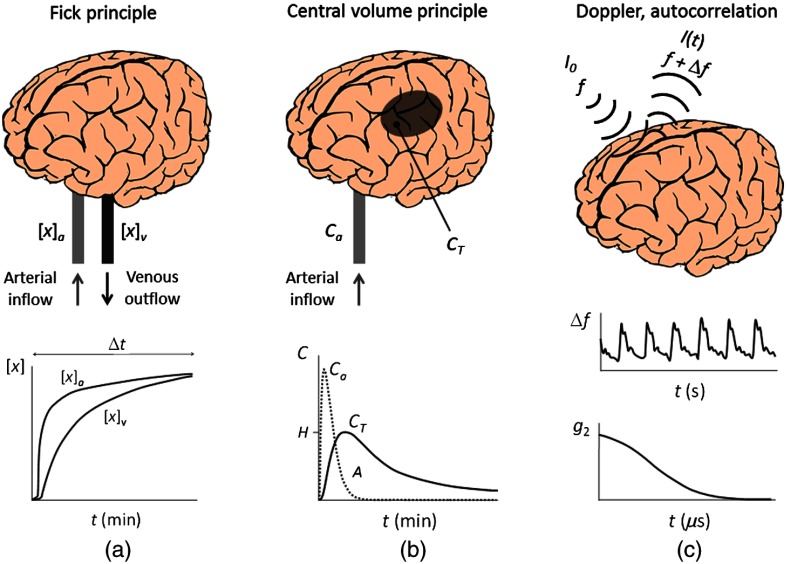
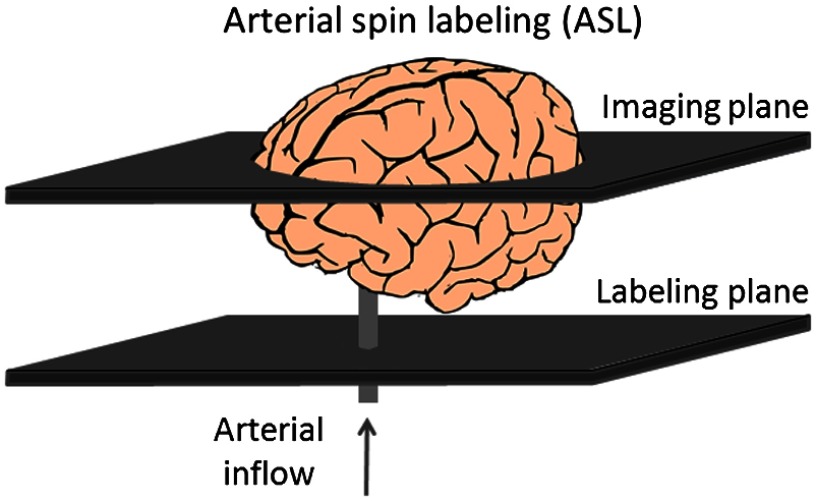
Cerebral blood flow (CBF) and cerebral autoregulation (CA) are critically important to maintain proper brain perfusion and supply the brain with the necessary oxygen and energy substrates. Adequate brain perfusion is required to support normal brain function, to achieve successful aging, and to navigate acute and chronic medical conditions. We review the general principles of CBF measurements and the current techniques to measure CBF based on direct intravascular measurements, nuclear medicine, X-ray imaging, magnetic resonance imaging, ultrasound techniques, thermal diffusion, and optical methods. We also review techniques for arterial blood pressure measurements as well as theoretical and experimental methods for the assessment of CA, including recent approaches based on optical techniques. The assessment of cerebral perfusion in the clinical practice is also presented. The comprehensive description of principles, methods, and clinical requirements of CBF and CA measurements highlights the potentially important role that noninvasive optical methods can play in the assessment of neurovascular health. In fact, optical techniques have the ability to provide a noninvasive, quantitative, and continuous monitor of CBF and autoregulation.
Keywords: Cerebral perfusion; autoregulation; coherent hemodynamics spectroscopy; computed tomography perfusion; diffuse correlation spectroscopy; laser Doppler flowmetry; near-infrared spectroscopy; perfusion magnetic resonance imaging; transcranial Doppler.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
