

Mortality Trends of Acute Respiratory Distress Syndrome in the United States from 1999 to 2013
- PMID: 27403914
- PMCID: PMC5122485
- DOI: 10.1513/AnnalsATS.201512-841OC
Mortality Trends of Acute Respiratory Distress Syndrome in the United States from 1999 to 2013
Abstract
Rationale: Acute respiratory distress syndrome (ARDS) is an acute hypoxemic respiratory failure seen in critically ill patients after an inciting injury. The burden of ARDS mortality in the United States in recent years is not well characterized.
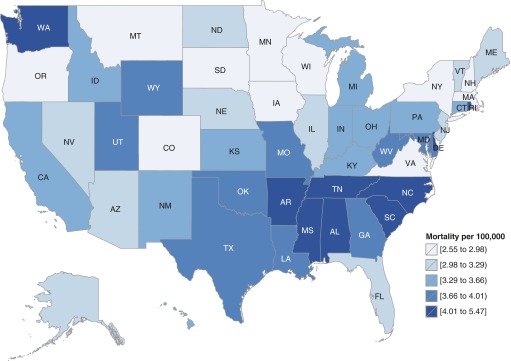
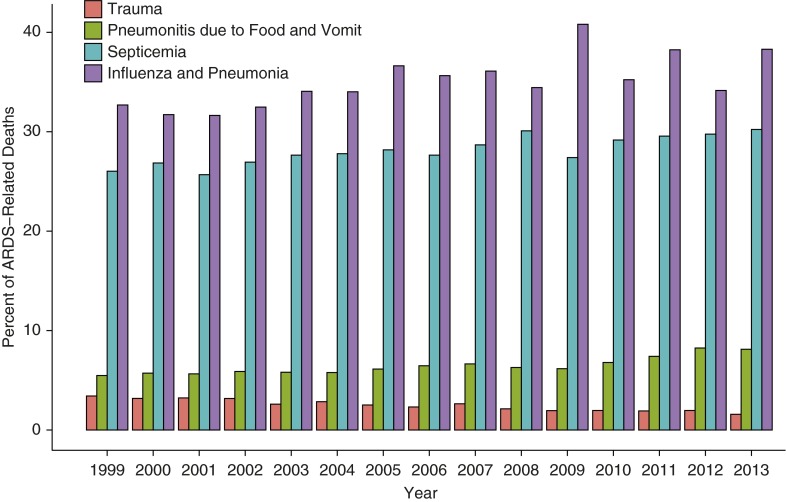
Objectives: In this study, we aimed to describe trends in the annual incidence of ARDS mortality in the United States from 1999 to 2013. We also describe demographic characteristics, geographic and seasonal trends, and other associated underlying causes of death in this population.
Methods: Data on all deceased U.S. residents are available through the Multiple Cause of Death (MCOD) database of the National Center for Health Statistics. ARDS-related deaths were identified in the MCOD database using International Classification of Diseases, 10th Revision.
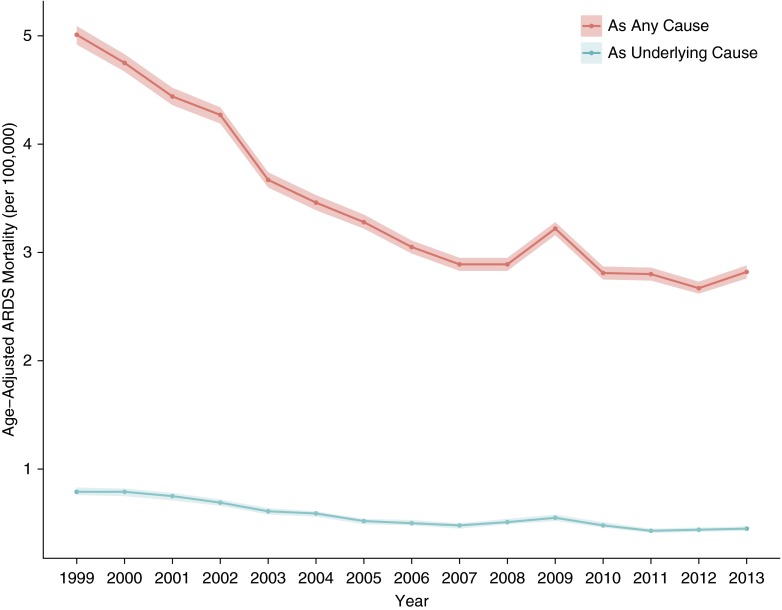
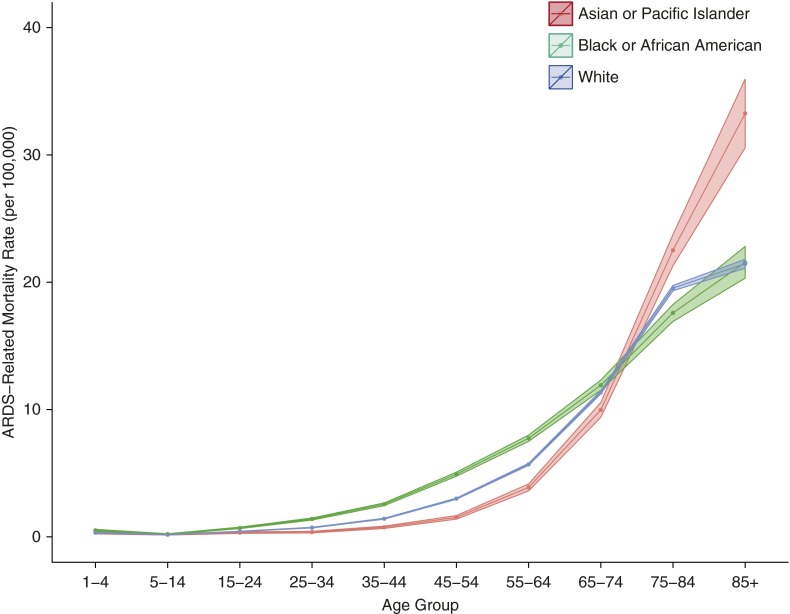
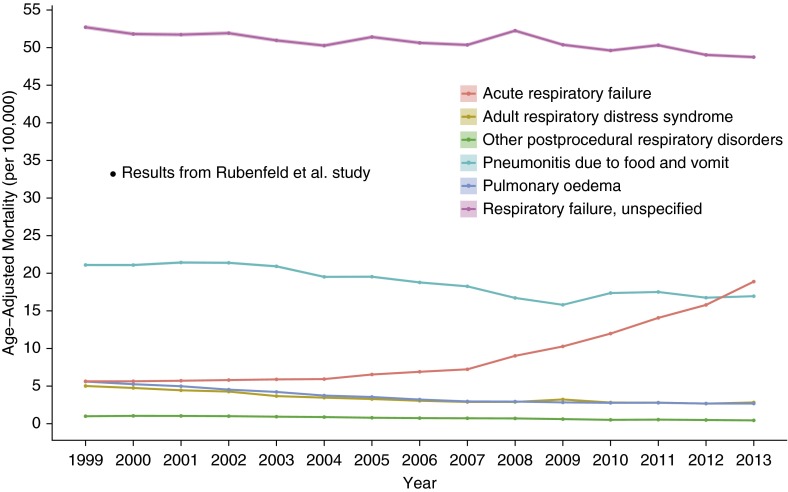
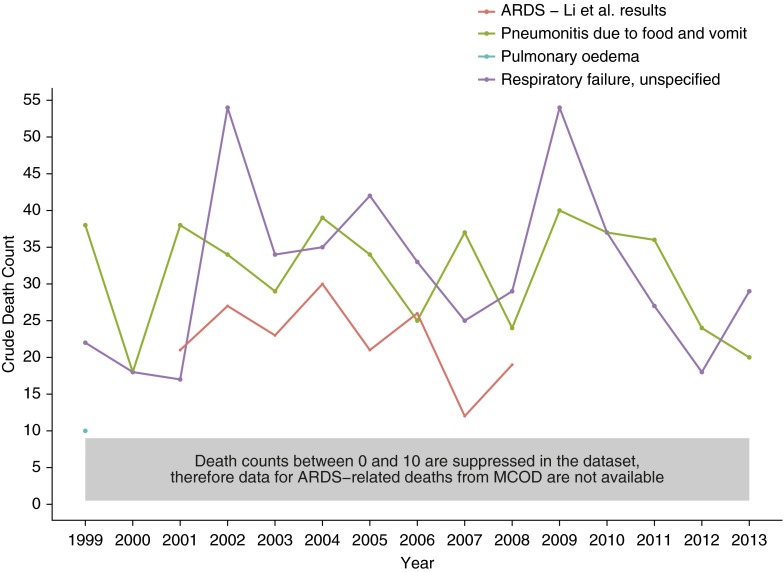
Measurements and main results: Aggregate annual crude and age-adjusted mortality rates and mortality rate ratios were used to compare various demographic subpopulations. Over the 15-year period, the national ARDS-related age-adjusted mortality rate demonstrated an annual seasonal variation, peaking in winter. The annual rate decreased in a nonlinear fashion, with a plateau from 2010 to 2013. The ARDS-related age-adjusted mortality rate was 5.01 per 100,000 persons (95% confidence interval, 4.92-5.09) in 1999 and 2.82 per 100,000 persons (95% confidence interval, 2.76-2.88) in 2013. Males had a higher average ARDS-related mortality rate than did females. Asian/Pacific Islanders had the lowest average age-adjusted ARDS-related mortality rate, and black/African-American individuals, the highest.
Conclusions: National age-adjusted ARDS-related mortality rates decreased between 1999 and 2013 in the United States, yet still show relative racial and sex disparities. However, death certificates largely underestimate the overall mortality burden from ARDS when compared with studies of clinically ascertained cases.
Keywords: acute lung injury; acute respiratory distress syndrome; critical care; critical illness; epidemiology.
Figures
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS ARDS Definition Task Force. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526–2533. - PubMed
-
- Wheeler AP, Bernard GR. Acute lung injury and the acute respiratory distress syndrome: a clinical review. Lancet. 2007;369:1553–1564. - PubMed
-
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, LeGall JR, Morris A, Spragg R The Consensus Committee. Report of the American-European consensus conference on ARDS: definitions, mechanisms, relevant outcomes and clinical trial coordination. Intensive Care Med. 1994;20:225–232. - PubMed
-
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet. 1967;2:319–323. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
