

Association Between Hospital Performance on Patient Safety and 30-Day Mortality and Unplanned Readmission for Medicare Fee-for-Service Patients With Acute Myocardial Infarction
- PMID: 27405808
- PMCID: PMC5015406
- DOI: 10.1161/JAHA.116.003731
Association Between Hospital Performance on Patient Safety and 30-Day Mortality and Unplanned Readmission for Medicare Fee-for-Service Patients With Acute Myocardial Infarction
Abstract
Background: Little is known regarding the relationship between hospital performance on adverse event rates and hospital performance on 30-day mortality and unplanned readmission rates for Medicare fee-for-service patients hospitalized for acute myocardial infarction (AMI).
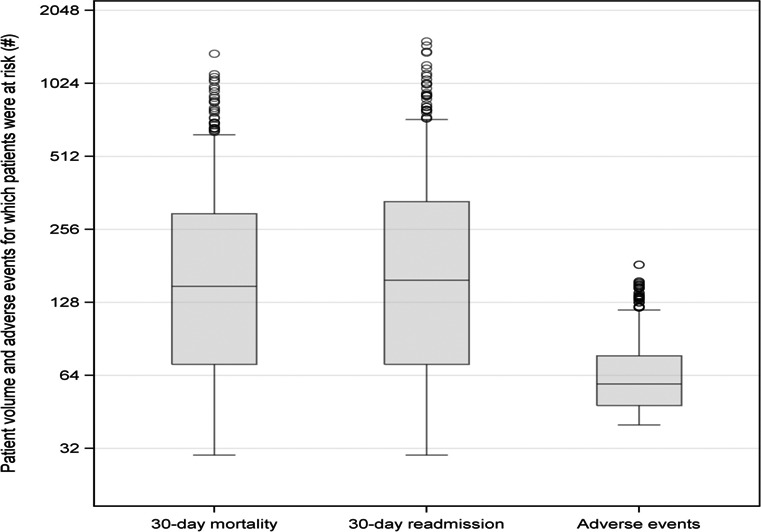
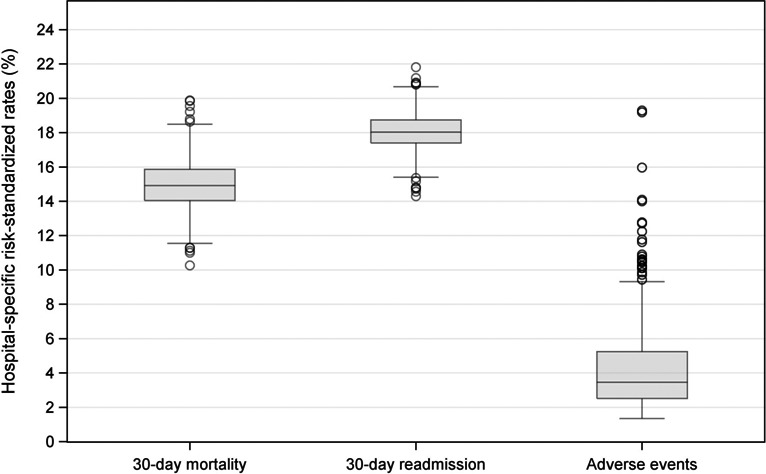
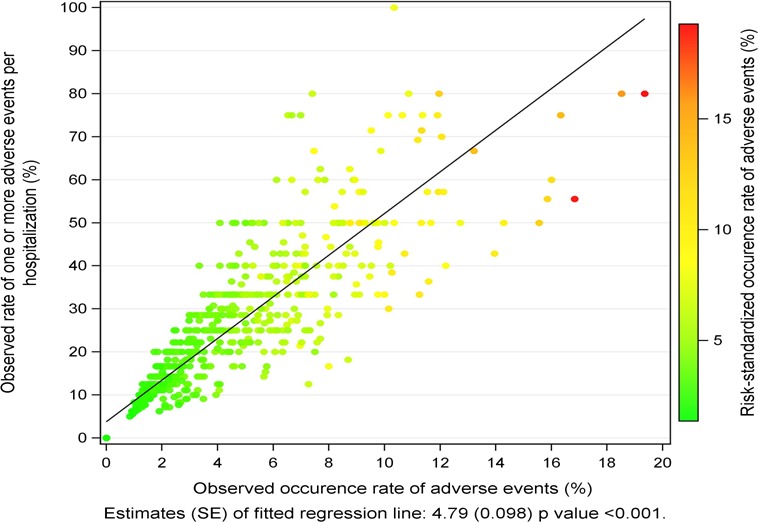
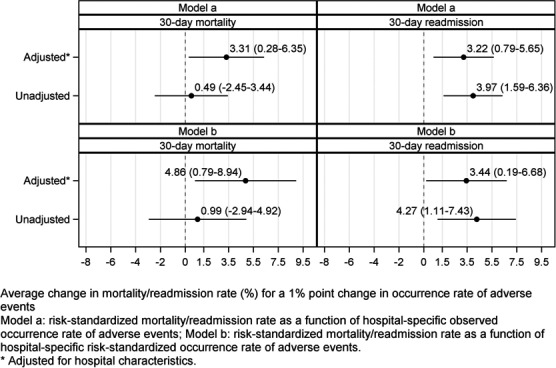
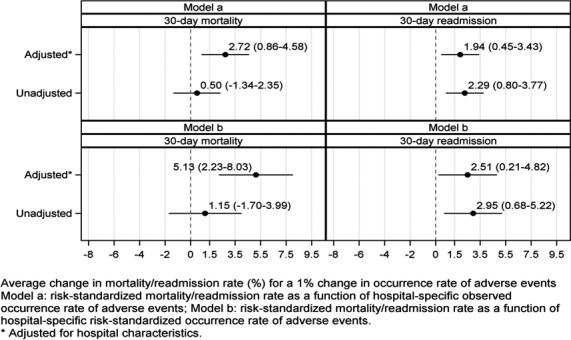
Methods and results: Using 2009-2013 medical record-abstracted patient safety data from the Agency for Healthcare Research and Quality's Medicare Patient Safety Monitoring System and hospital mortality and readmission data from the Centers for Medicare & Medicaid Services, we fitted a mixed-effects model, adjusting for hospital characteristics, to evaluate whether hospital performance on patient safety, as measured by the hospital-specific risk-standardized occurrence rate of 21 common adverse event measures for which patients were at risk, is associated with hospital-specific 30-day all-cause risk-standardized mortality and unplanned readmission rates for Medicare patients with AMI. The unit of analysis was at the hospital level. The final sample included 793 acute care hospitals that treated 30 or more Medicare patients hospitalized for AMI and had 40 or more adverse events for which patients were at risk. The occurrence rate of adverse events for which patients were at risk was 3.8%. A 1% point change in the risk-standardized occurrence rate of adverse events was associated with average changes in the same direction of 4.86% points (95% CI, 0.79-8.94) and 3.44% points (95% CI, 0.19-6.68) for the risk-standardized mortality and unplanned readmission rates, respectively.
Conclusions: For Medicare fee-for-service patients discharged with AMI, hospitals with poorer patient safety performance were also more likely to have poorer performance on 30-day all-cause mortality and on unplanned readmissions.
Keywords: Medicare; mortality; myocardial infarction; patient safety; readmission.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Institute of Medicine report, patient safety: achieving a new standard for care. Acad Emerg Med. 2005;12:1011–1012. - PubMed
-
- Leape L, Berwick D. Five years after to Err is human—what have we learned. JAMA. 2005;293:2384–2390. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- Berenson RA, Paulus RA, Kalman NS. Medicare's readmissions‐reduction program–a positive alternative. N Engl J Med. 2012;366:1364–1366. - PubMed
-
- Joynt KE, Jha AK. Thirty‐day readmissions—truth or consequences. N Engl J Med. 2012;366:1366–1369. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
