

The economic burden of asthma and chronic obstructive pulmonary disease and the impact of poor inhalation technique with commonly prescribed dry powder inhalers in three European countries
- PMID: 27406133
- PMCID: PMC4942909
- DOI: 10.1186/s12913-016-1482-7
The economic burden of asthma and chronic obstructive pulmonary disease and the impact of poor inhalation technique with commonly prescribed dry powder inhalers in three European countries
Abstract
Background: Asthma and chronic obstructive pulmonary disease (COPD) are common chronic inflammatory respiratory diseases, which impose a substantial burden on healthcare systems and society. Fixed-dose combinations (FDCs) of inhaled corticosteroids (ICS) and long-acting β2 agonists (LABA), often administered using dry powder inhalers (DPIs), are frequently prescribed to control persistent asthma and COPD. Use of DPIs has been associated with poor inhalation technique, which can lead to increased healthcare resource use and costs.
Methods: A model was developed to estimate the healthcare resource use and costs associated with asthma and COPD management in people using commonly prescribed DPIs (budesonide + formoterol Turbuhaler(®) or fluticasone + salmeterol Accuhaler(®)) over 1 year in Spain, Sweden and the United Kingdom (UK). The model considered direct costs (inhaler acquisition costs and scheduled and unscheduled healthcare costs), indirect costs (productive days lost), and estimated the contribution of poor inhalation technique to the burden of illness.
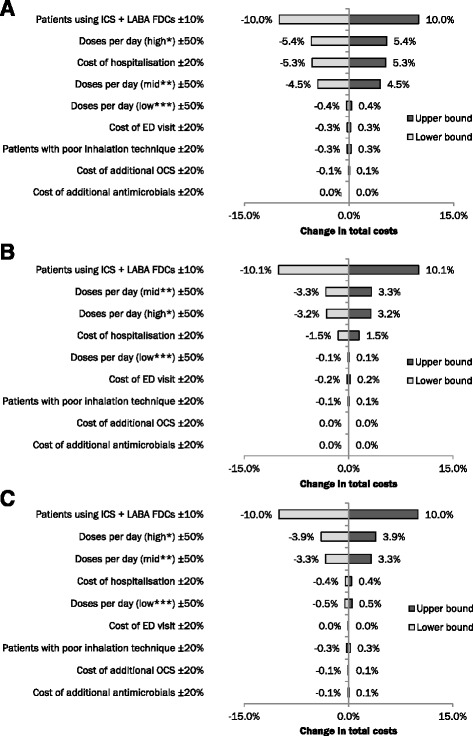
Results: The direct cost burden of managing asthma and COPD for people using budesonide + formoterol Turbuhaler(®) or fluticasone + salmeterol Accuhaler(®) in 2015 was estimated at €813 million, €560 million, and €774 million for Spain, Sweden and the UK, respectively. Poor inhalation technique comprised 2.2-7.7 % of direct costs, totalling €105 million across the three countries. When lost productivity costs were included, total expenditure increased to €1.4 billion, €1.7 billion and €3.3 billion in Spain, Sweden and the UK, respectively, with €782 million attributable to poor inhalation technique across the three countries. Sensitivity analyses showed that the model results were most sensitive to changes in the proportion of patients prescribed ICS and LABA FDCs, and least sensitive to differences in the number of antimicrobials and oral corticosteroids prescribed.
Conclusions: The cost of managing asthma and COPD using commonly prescribed DPIs is considerable. A substantial, and avoidable, contributor to this burden is poor inhalation technique. Measures that can improve inhalation technique with current DPIs, such as easier-to-use inhalers or better patient training, could offer benefits to patients and healthcare providers through improving disease outcomes and lowering costs.
Keywords: Asthma; Burden of illness; COPD; Cost; DPI; Model; Poor inhalation technique.
Figures


References
-
- World Health Organization. World Health Survey. Available from: www.who.int/healthinfo/survey/en/. Accessed: Jan 2012.
-
- European Respiratory Society (ERS). Assessing asthma quality of life: its role in clinical practice. Available from: http://www.ers-education.org/lrMedia/2005/pdf/40500.pdf. Accessed: Nov 2013
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
