

A randomized phase II trial of standard dose bevacizumab versus low dose bevacizumab plus lomustine (CCNU) in adults with recurrent glioblastoma
- PMID: 27406589
- PMCID: PMC5021605
- DOI: 10.1007/s11060-016-2195-9
A randomized phase II trial of standard dose bevacizumab versus low dose bevacizumab plus lomustine (CCNU) in adults with recurrent glioblastoma
Abstract
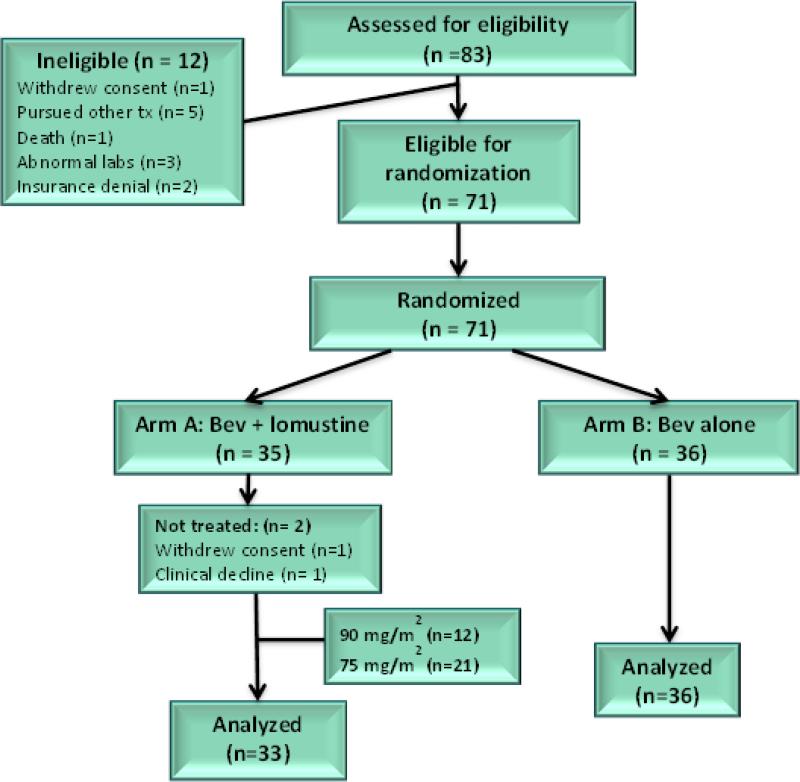
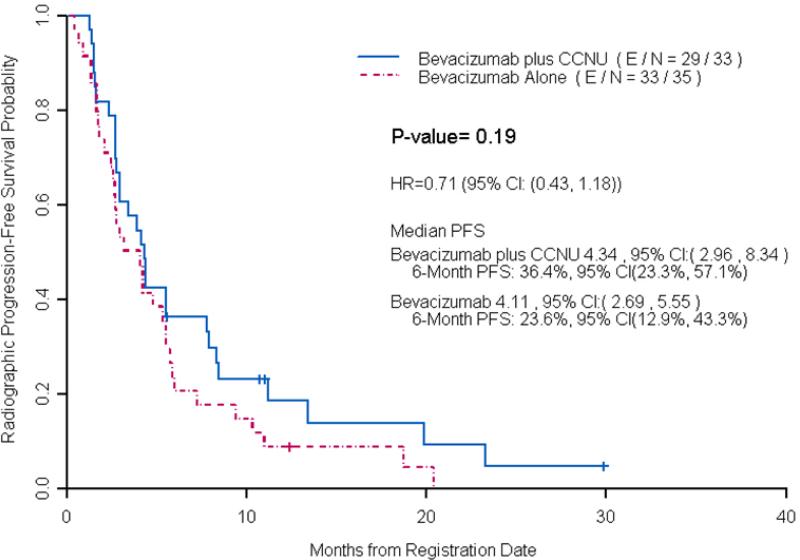
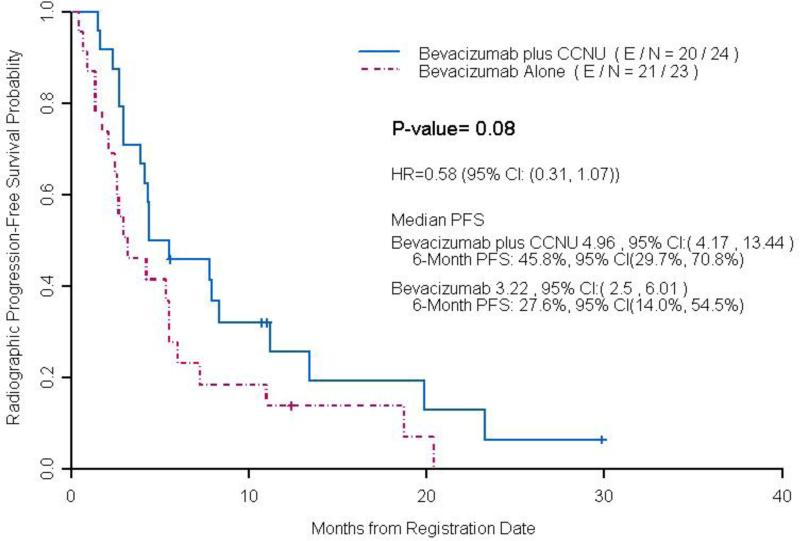
Antiangiogenic therapy can rapidly reduce vascular permeability and cerebral edema but high doses of bevacizumab may induce selective pressure to promote resistance. This trial evaluated the efficacy of low dose bevacizumab in combination with lomustine (CCNU) compared to standard dose bevacizumab in patients with recurrent glioblastoma. Patients (N = 71) with recurrent glioblastoma who previously received radiation and temozolomide were randomly assigned 1:1 to receive bevacizumab monotherapy (10 mg/kg) or low dose bevacizumab (5 mg/kg) in combination with lomustine (90 mg/m(2)). The primary end point was progression-free survival (PFS) based on a blinded, independent radiographic assessment of post-contrast T1-weighted and non-contrast T2/FLAIR weighted magnetic resonance imaging (MRI) using RANO criteria. For 69 evaluable patients, median PFS was not significantly longer in the low dose bevacizumab + lomustine arm (4.34 months, CI 2.96-8.34) compared to the bevacizumab alone arm (4.11 months, CI 2.69-5.55, p = 0.19). In patients with first recurrence, there was a trend towards longer median PFS time in the low dose bevacizumab + lomustine arm (4.96 months, CI 4.17-13.44) compared to the bevacizumab alone arm (3.22 months CI 2.5-6.01, p = 0.08). The combination of low dose bevacizumab plus lomustine was not superior to standard dose bevacizumab in patients with recurrent glioblastoma. Although the study was not designed to exclusively evaluate patients at first recurrence, a strong trend towards improved PFS was seen in that subgroup for the combination of low dose bevacizumab plus lomustine. Further studies are needed to better identify such subgroups that may most benefit from the combination treatment.
Keywords: Angiogenesis; Bevacizumab; Glioblastoma; Lomustine; VEGF.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005 Mar 10;352(10):987–996. - PubMed
-
- Wong ET, Hess KR, Gleason MJ, et al. Outcomes and prognostic factors in recurrent glioma patients enrolled onto phase II clinical trials. J Clin Oncol. 1999 Aug;17(8):2572–2578. - PubMed
-
- Carmeliet P. Angiogenesis in life, disease and medicine. Nature. 2005 Dec 15;438(7070):932–936. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
