

Complementary therapies for labour and birth study: a randomised controlled trial of antenatal integrative medicine for pain management in labour
- PMID: 27406639
- PMCID: PMC4947718
- DOI: 10.1136/bmjopen-2015-010691
Complementary therapies for labour and birth study: a randomised controlled trial of antenatal integrative medicine for pain management in labour
Erratum in
-
Correction: Complementary therapies for labour and birth study: a randomised controlled trial of antenatal integrative medicine for pain management in labour.BMJ Open. 2016 Nov 10;6(11):e010691corr1. doi: 10.1136/bmjopen-2015-010691corr1. BMJ Open. 2016. PMID: 28186952 Free PMC article. No abstract available.
Abstract
Objective: To evaluate the effect of an antenatal integrative medicine education programme in addition to usual care for nulliparous women on intrapartum epidural use.
Design: Open-label, assessor blind, randomised controlled trial.
Setting: 2 public hospitals in Sydney, Australia.
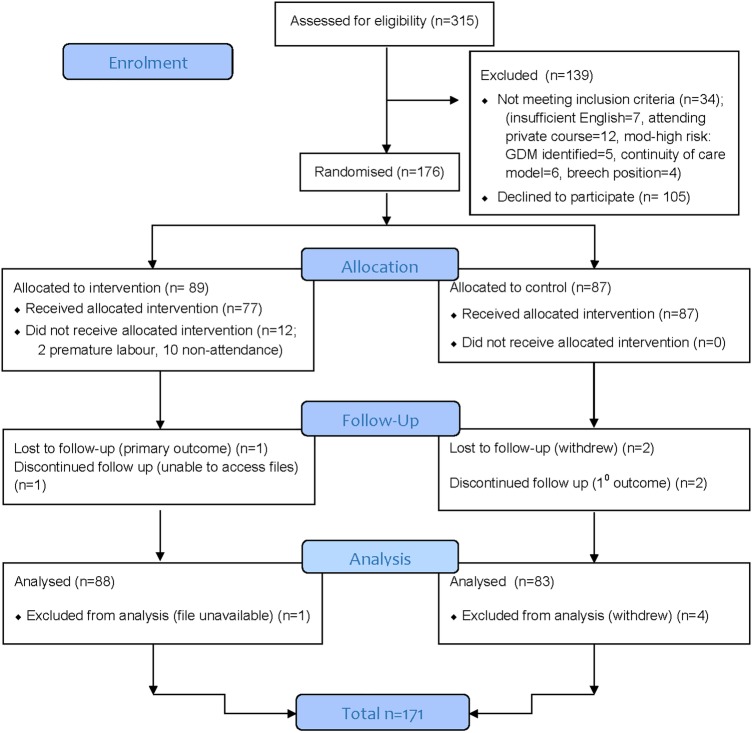
Population: 176 nulliparous women with low-risk pregnancies, attending hospital-based antenatal clinics.
Methods and intervention: The Complementary Therapies for Labour and Birth protocol, based on the She Births and acupressure for labour and birth courses, incorporated 6 evidence-based complementary medicine techniques: acupressure, visualisation and relaxation, breathing, massage, yoga techniques, and facilitated partner support. Randomisation occurred at 24-36 weeks' gestation, and participants attended a 2-day antenatal education programme plus standard care, or standard care alone.
Main outcome measures: Rate of analgesic epidural use. Secondary: onset of labour, augmentation, mode of birth, newborn outcomes.
Results: There was a significant difference in epidural use between the 2 groups: study group (23.9%) standard care (68.7%; risk ratio (RR) 0.37 (95% CI 0.25 to 0.55), p≤0.001). The study group participants reported a reduced rate of augmentation (RR=0.54 (95% CI 0.38 to 0.77), p<0.0001); caesarean section (RR=0.52 (95% CI 0.31 to 0.87), p=0.017); length of second stage (mean difference=-0.32 (95% CI -0.64 to 0.002), p=0.05); any perineal trauma (0.88 (95% CI 0.78 to 0.98), p=0.02) and resuscitation of the newborn (RR=0.47 (95% CI 0.25 to 0.87), p≤0.015). There were no statistically significant differences found in spontaneous onset of labour, pethidine use, rate of postpartum haemorrhage, major perineal trauma (third and fourth degree tears/episiotomy), or admission to special care nursery/neonatal intensive care unit (p=0.25).
Conclusions: The Complementary Therapies for Labour and Birth study protocol significantly reduced epidural use and caesarean section. This study provides evidence for integrative medicine as an effective adjunct to antenatal education, and contributes to the body of best practice evidence.
Trial registration number: ACTRN12611001126909.
Keywords: COMPLEMENTARY MEDICINE; Caesarean section; Epidural; antenatal education; normal birth; randomised controlled trial.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
References
-
- Gibbons L, Belizán JM, Lauer JA et al. The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: overuse as a barrier to universal coverage. World Health Rep 2010;30:1–31.
-
- WHO. Caesarean sections should only be performed when medically necessary. Executive summary. In: WHO , ed. Geneva: WHO, 2015:8.
-
- Bryant R. Improving maternity services in Australia: the report of the maternity services review. In: Australia Co , ed. Canberra: Commonwealth of Australia, 2009.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical