

Differential host susceptibility and bacterial virulence factors driving Klebsiella liver abscess in an ethnically diverse population
- PMID: 27406977
- PMCID: PMC4942785
- DOI: 10.1038/srep29316
Differential host susceptibility and bacterial virulence factors driving Klebsiella liver abscess in an ethnically diverse population
Abstract
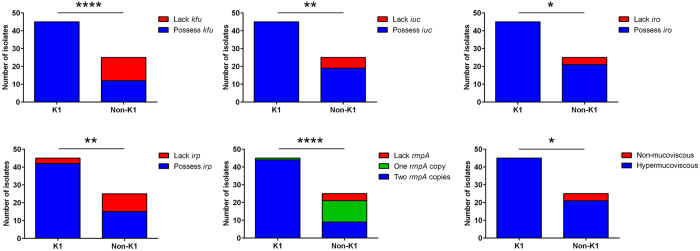
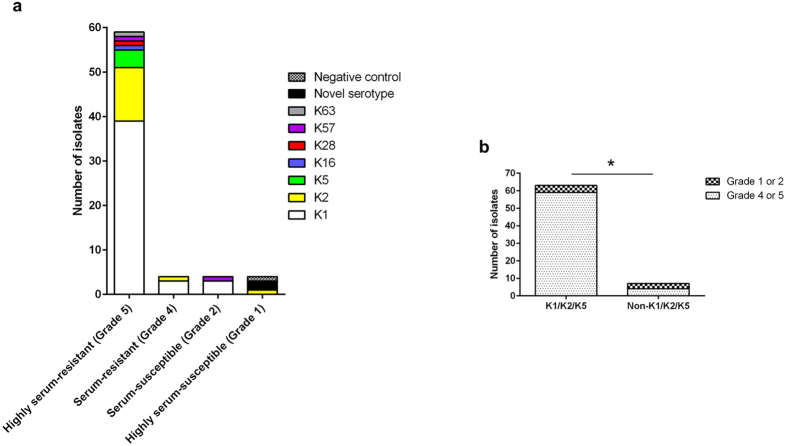
Hypervirulent Klebsiella pneumoniae is an emerging cause of community-acquired pyogenic liver abscess. First described in Asia, it is now increasingly recognized in Western countries, commonly afflicting those with Asian descent. This raises the question of genetic predisposition versus geospecific strain acquisition. We leveraged on the Antibiotics for Klebsiella Liver Abscess Syndrome Study (A-KLASS) clinical trial ongoing in ethnically diverse Singapore, to prospectively examine the profiles of 70 patients together with their isolates' genotypic and phenotypic characteristics. The majority of isolates belonged to capsule type K1, a genetically homogenous group corresponding to sequence-type 23. The remaining K2, K5, K16, K28, K57 and K63 isolates as well as two novel cps isolates were genetically heterogeneous. K1 isolates carried higher frequencies of virulence-associated genes including rmpA (regulator of mucoid phenotype A), kfu (Klebsiella ferric uptake transporter), iuc (aerobactin), iro (salmochelin) and irp (yersiniabactin) than non-K1 isolates. The Chinese in our patient cohort, mostly non-diabetic, had higher prevalence of K1 infection than the predominantly diabetic non-Chinese (Malays, Indian and Caucasian). This differential susceptibility to different capsule types among the various ethnic groups suggests patterns of transmission (e.g. environmental source, familial transmission) and/or genetic predisposition unique to each race despite being in the same geographical location.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
