

Immunophenotyping of Tumours
- PMID: 27408072
- PMCID: PMC4921750
- DOI: 10.1016/S0377-1237(08)80138-4
Immunophenotyping of Tumours
Abstract
Background: Immunophenotyping has added a new dimension to improve the diagnostic accuracy of malignant diseases. The emphasis is on its usefulness in planning and institution of specific therapy besides helping in prognostication.
Methods: The study included 83/1385 biopsies of cancer patients over an 18 month period on which immunohistochemical staining (IHC) with monoclonal antibodies were performed. The technique was used to establish the histogenetic origins/expression of the tumours. The study excluded haematolymphoid malignancies.
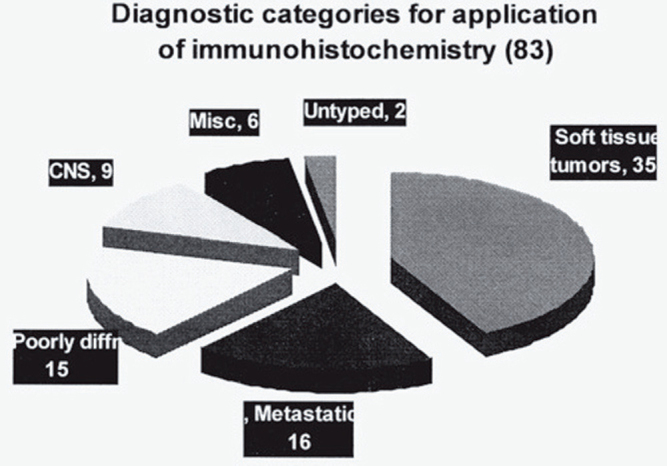
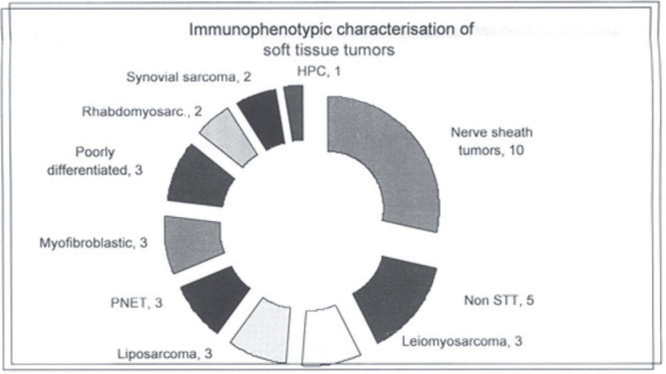
Result: Eighty three cases on whom IHC was performed included poorly differentiated tumours (15), metastatic tumours (16), soft tissue tumours (35), central nervous system tumours (9) and miscellaneous (6). Two cases could not be typed. The clinicopathological correlation in terms of the management and the problems related to its misinterpretation are discussed.
Conclusion: Immunophenotyping of tumours in an oncology set up is significant in the 'Final Diagnosis'.
Keywords: Diagnosis; Immunophenotyping; Tumour markers.
Figures
Similar articles
-
The EGF receptor system in head and neck carcinomas and normal tissues. Immunohistochemical and quantitative studies.Dan Med Bull. 1998 Apr;45(2):121-34. Dan Med Bull. 1998. PMID: 9587699 Review.
-
Immunophenotype, ras oncogenes and p53 onco-suppressor gene in benzo(a)pyrene induced malignant soft tissue tumours in Wistar rats.In Vivo. 1998 Sep-Oct;12(5):511-21. In Vivo. 1998. PMID: 9827359
-
Italian cancer figures, report 2012: Cancer in children and adolescents.Epidemiol Prev. 2013 Jan-Feb;37(1 Suppl 1):1-225. Epidemiol Prev. 2013. PMID: 23585445 English, Italian.
-
Italian cancer figures--Report 2015: The burden of rare cancers in Italy.Epidemiol Prev. 2016 Jan-Feb;40(1 Suppl 2):1-120. doi: 10.19191/EP16.1S2.P001.035. Epidemiol Prev. 2016. PMID: 26951748
-
Gastrointestinal carcinoid tumours. Histogenetic, histochemical, immunohistochemical, clinical and therapeutic aspects.Prog Histochem Cytochem. 1989;19(2):1-88. Prog Histochem Cytochem. 1989. PMID: 2662260 Review.
References
-
- Wick MR, Ritter JH, Swanson PE. The impact of diagnostic immunohistochemistry on patient outcomes. Clin Lab Med. 1999;19:814–907. - PubMed
-
- Taylor CR. The current role of immunohistochemistry in diagnostic pathology. Adv Pathol Lab Med. 1994;7:59–65.
-
- Taylor CR. The total test approach to standardization of immunohistochemistry. Arch Pathol Lab Med. 2000;124:945–951. - PubMed
-
- Shi SR, Cote RJ, Taylor CR. Antigen retrieval techniques: current perspectives. J Histochem Cytochem. 2001;49:931–937. - PubMed
-
- Hammar SP. Metastatic adenocarcinoma of unknown primary origin. Hum Pathol. 1998;29:1393–1402. - PubMed
LinkOut - more resources
Full Text Sources
