

Case Reports
doi: 10.2484/rcr.v10i1.1010.
eCollection 2015.
Primary intramedullary melanocytoma in the cervical spinal cord: Case report and literature review
- PMID: 27408655
- PMCID: PMC4921164
- DOI: 10.2484/rcr.v10i1.1010
Item in Clipboard
Case Reports
Primary intramedullary melanocytoma in the cervical spinal cord: Case report and literature review
Radiol Case Rep.
.
Abstract
A 63-year-old man with right hemiparesis was found (on MRI) to have an expansive intramedullary tumorous lesion at the C2-C3 level. After complete neurosurgical tumor resection, the tumor was histologically categorized as an intermediate grade of intramedullary melanocytoma, an uncommon neoplasm. Based on this peculiar case and review of the literature, radical surgical resection appears to be the therapy of choice for intramedullary melanocytomas. However, their high recurrence rate and aggressive behavior suggest the need for close followup with serial MRI.
Figures
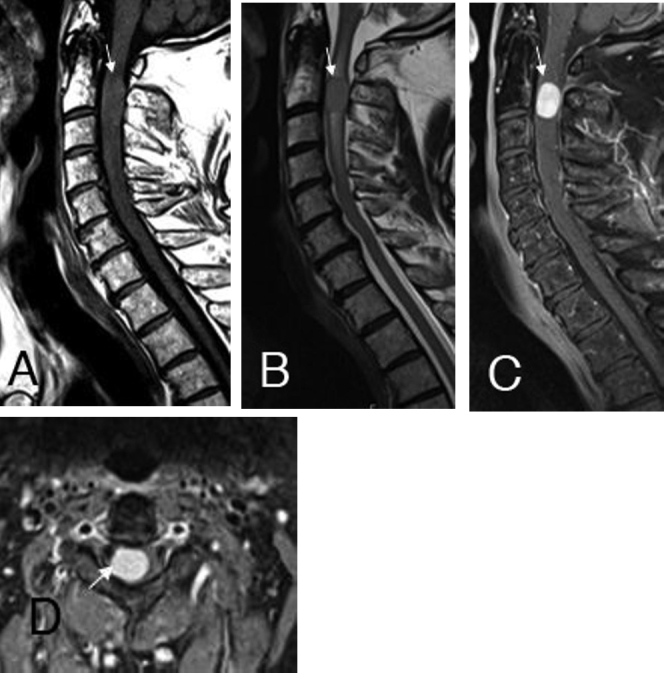
The sagittal T1- (A) and T2-weighted (B) images and the postcontrast sagittal (C) and axial (D) fat-suppressed T1-weighted images clearly show the intramedullary, paracentral right located, expansive melanocytoma at the C2 / C3 level with homogeneous contrast enhancement. Additionally, a T2w hyperintense (B) per focal tumoral edema was noticed, suggestive of myelopathy.
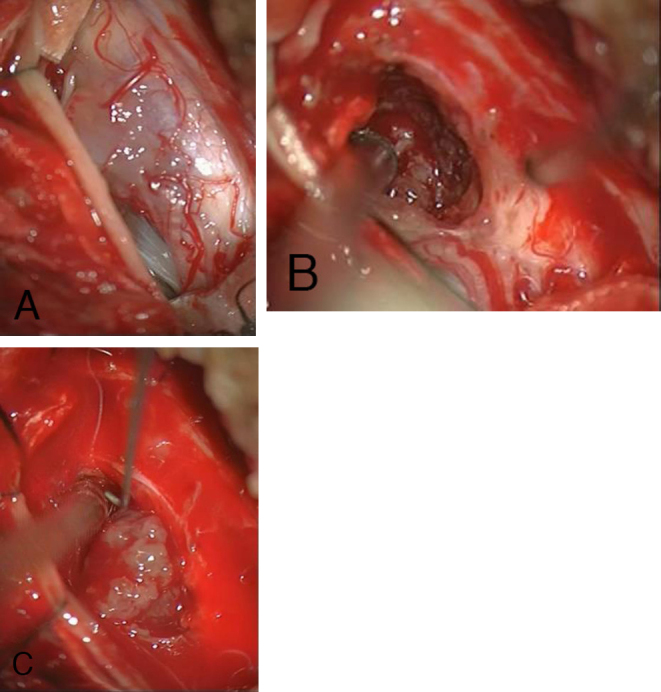
Intraoperative view of the spinal cord after opening the dura mater via dorsal laminectomy; the tumor shines brightly in (A). Melanocytoma with visible caudal tumor edge (B) and partially dissected melanocytoma (C).
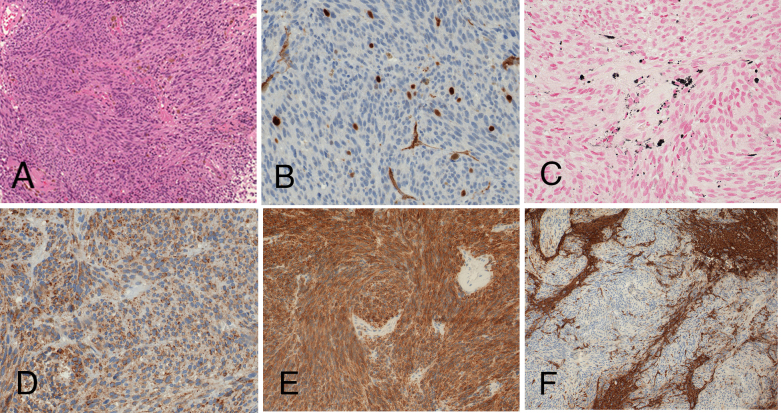
Histological examination revealed a melanocytic neoplasm with moderate mitotic activity and infiltrative growth pattern. Conventional hematoxilin and eosin staining (A; x100) shows lack of substantial cytologic atypia; a mitotic figure is depicted in the inset. Moderate MIB1 staining supports higher proliferative potential (B; x400). Melanocytic differentiation is disclosed by melanin pigmentation (C; Fontana-Masson staining, x400), and immunohistochemical positivity for the melanocytic markers HMB45 (D; x400) and Melan A (E; x200). Staining for glial fibrillary acidic protein (F; GFAP, x100) highlights the invasive tumor growth pattern, with unstained tumor cells and positively stained infiltrated central nervous tissue.
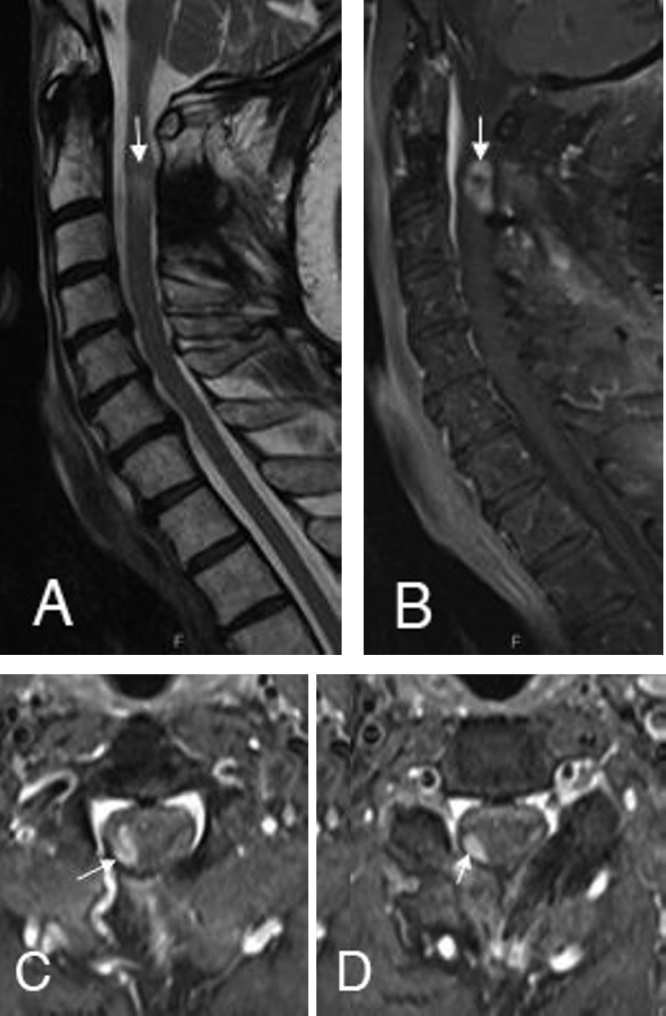
The followup MRI after 3 months indicates the solid enhancing tumor recurrence (B) at the right adherent lateral resection border at the C2 (C) and C3 level (D). The signs of cervical myelopathy were still recognizable on the sagittal T2-weighted (A) images.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
