

The role of spontaneous effort during mechanical ventilation: normal lung versus injured lung
- PMID: 27408729
- PMCID: PMC4940771
- DOI: 10.1186/s40560-015-0083-6
The role of spontaneous effort during mechanical ventilation: normal lung versus injured lung
Abstract
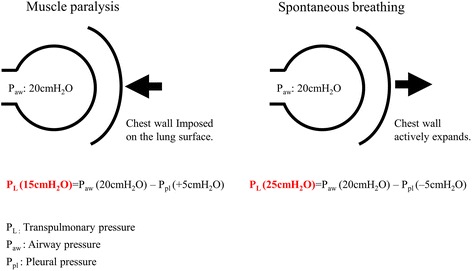
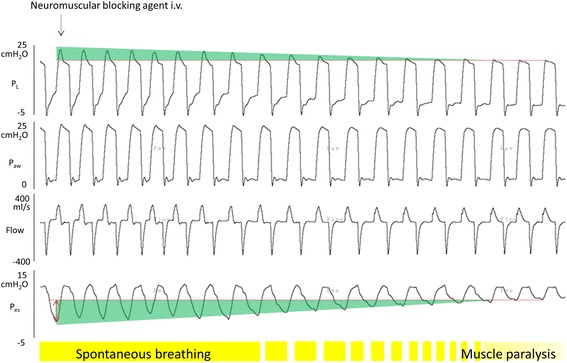
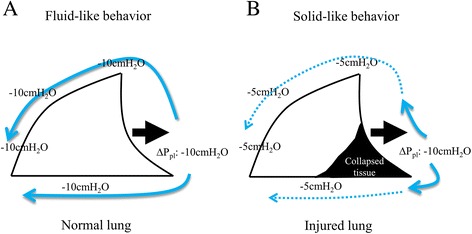
The role of preserving spontaneous effort during mechanical ventilation and its interaction with mechanical ventilation have been actively investigated for several decades. Inspiratory muscle activities can lower the pleural components surrounding the lung, leading to an increase in transpulmonary pressure when spontaneous breathing effort is preserved during mechanical ventilation. Thus, increased transpulmonary pressure provides various benefits for gas exchange, ventilation pattern, and lung aeration. However, it is important to note that these beneficial effects of preserved spontaneous effort have been demonstrated only when spontaneous effort is modest and lung injury is less severe. Recent studies have revealed the 'dark side' of spontaneous effort during mechanical ventilation, especially in severe lung injury. The 'dark side' refers to uncontrollable transpulmonary pressure due to combined high inspiratory pressure with excessive spontaneous effort and the injurious lung inflation pattern of Pendelluft (i.e., the translocation of air from nondependent lung regions to dependent lung regions). Thus, during the early stages of severe ARDS, the strict control of transpulmonary pressure and prevention of Pendelluft should be achieved with the short-term use of muscle paralysis. When there is preserved spontaneous effort in ARDS, spontaneous effort should be maintained at a modest level, as the transpulmonary pressure and the effect size of Pendelluft depend on the intensity of the spontaneous effort.
Keywords: ARDS; Lung injury; Muscle paralysis; Pendelluft; Pleural pressure; Spontaneous breathing; Transpulmonary pressure.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
