

Imaging Foveal Microvasculature: Optical Coherence Tomography Angiography Versus Adaptive Optics Scanning Light Ophthalmoscope Fluorescein Angiography
- PMID: 27409463
- PMCID: PMC4968918
- DOI: 10.1167/iovs.15-18932
Imaging Foveal Microvasculature: Optical Coherence Tomography Angiography Versus Adaptive Optics Scanning Light Ophthalmoscope Fluorescein Angiography
Abstract
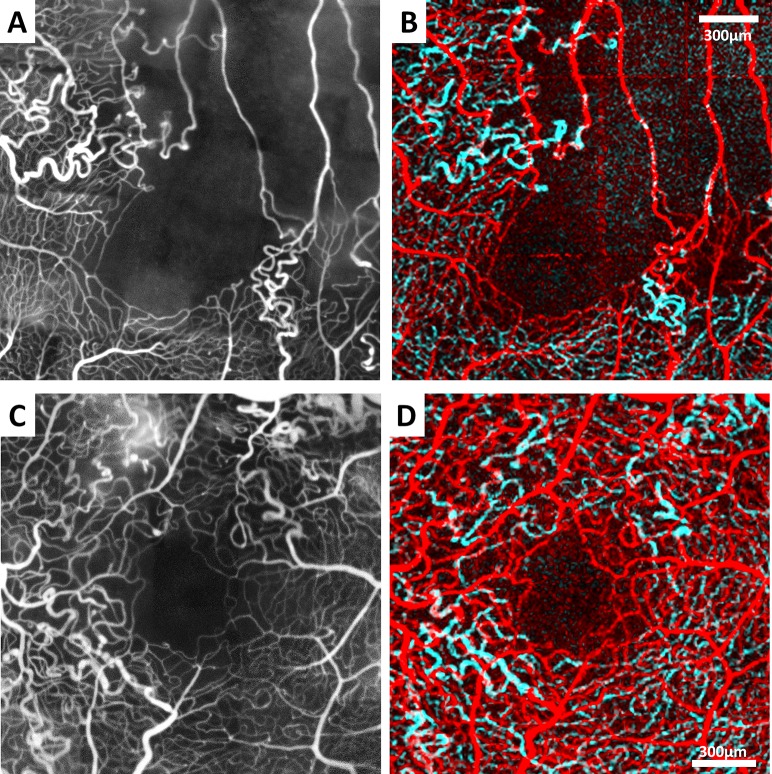
Purpose: To compare the use of optical coherence tomography angiography (OCTA) and adaptive optics scanning light ophthalmoscope fluorescein angiography (AOSLO FA) for characterizing the foveal microvasculature in healthy and vasculopathic eyes.
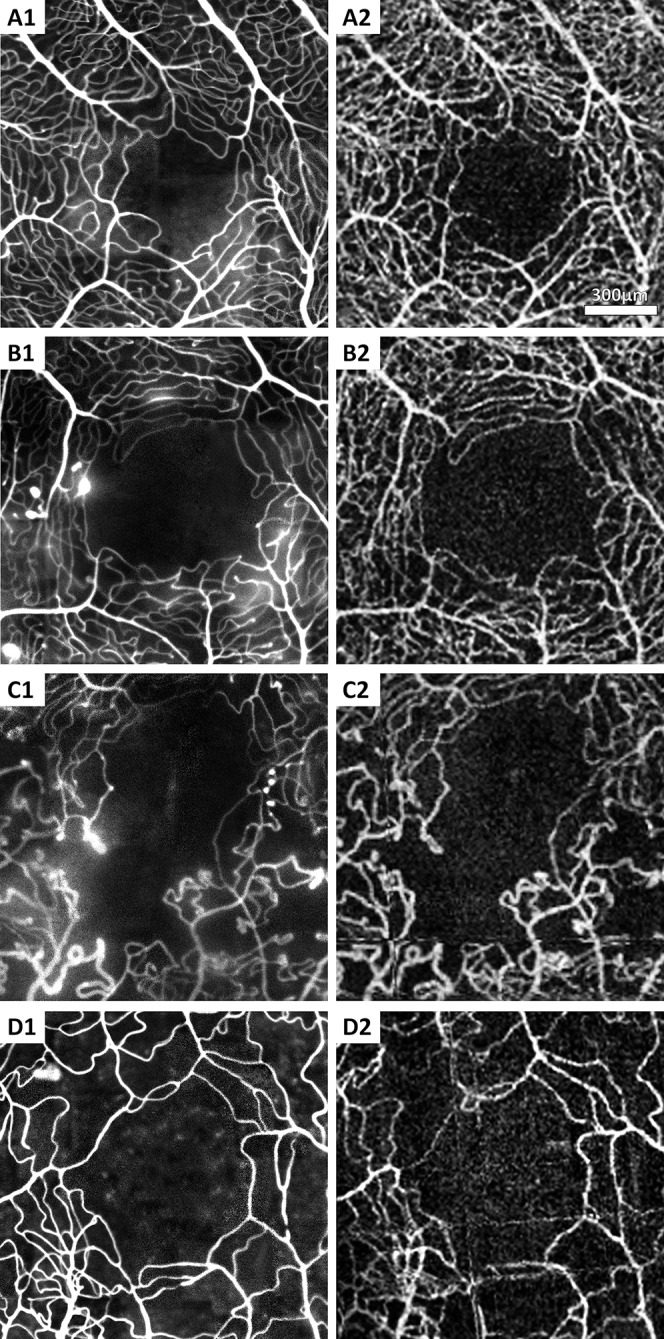
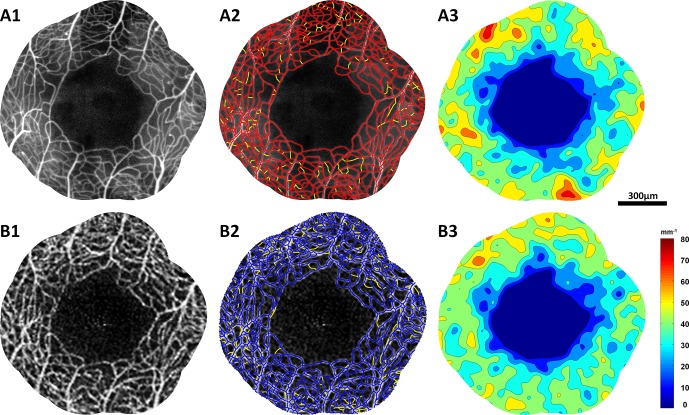
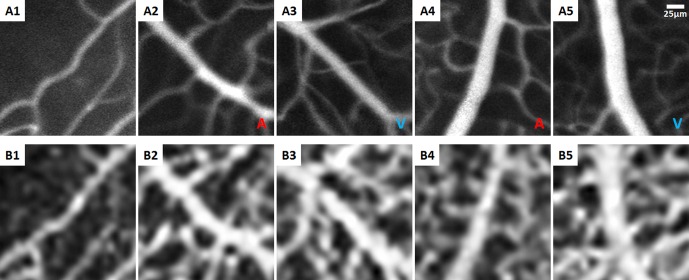
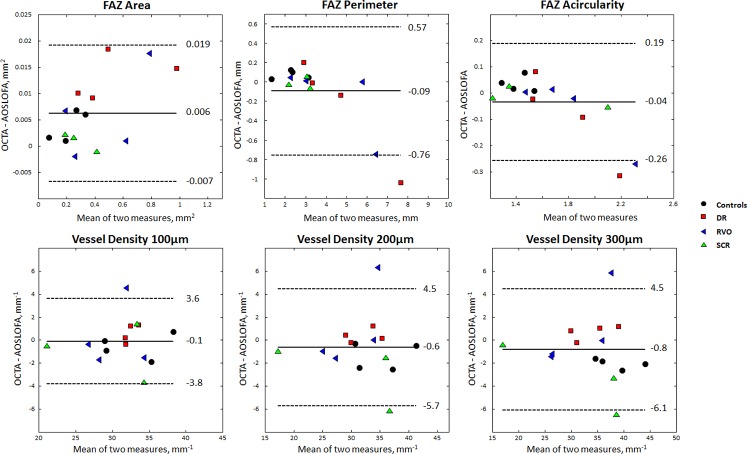
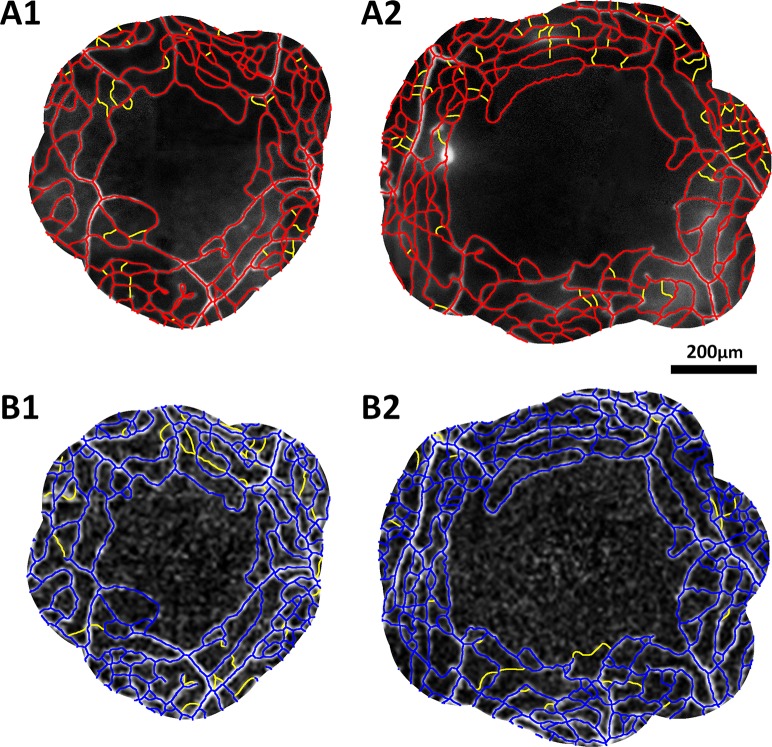
Methods: Four healthy controls and 11 vasculopathic patients (4 diabetic retinopathy, 4 retinal vein occlusion, and 3 sickle cell retinopathy) were imaged with OCTA and AOSLO FA. Foveal perfusion maps were semiautomatically skeletonized for quantitative analysis, which included foveal avascular zone (FAZ) metrics (area, perimeter, acircularity index) and vessel density in three concentric annular regions of interest. On each set of OCTA and AOSLO FA images, matching vessel segments were used for lumen diameter measurement. Qualitative image comparisons were performed by visual identification of microaneurysms, vessel loops, leakage, and vessel segments.
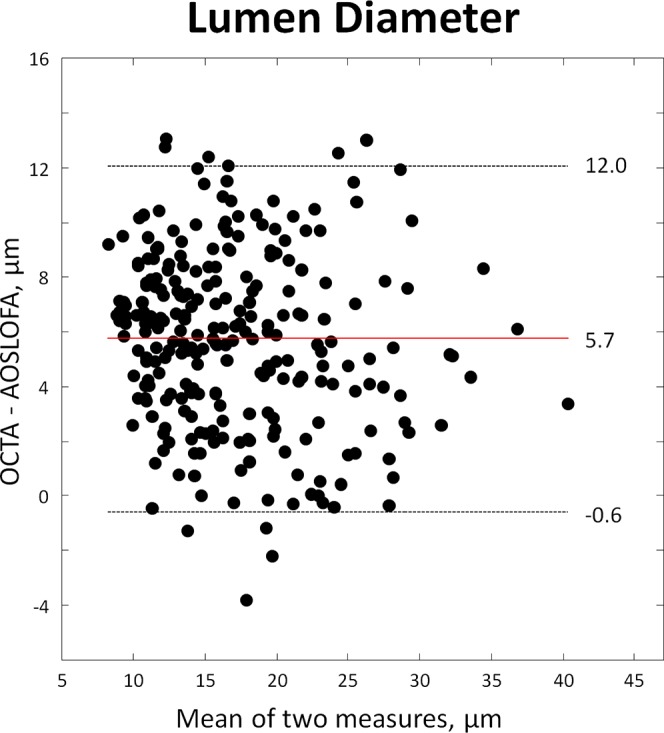
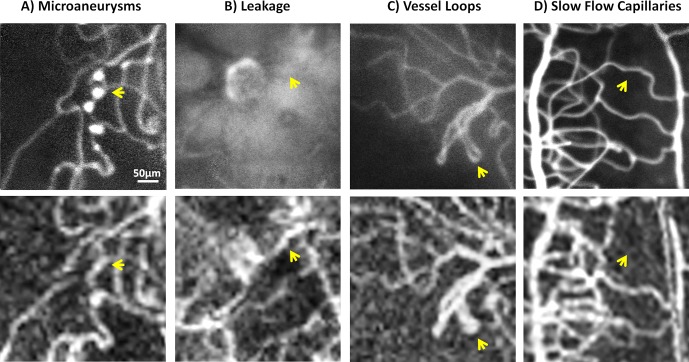
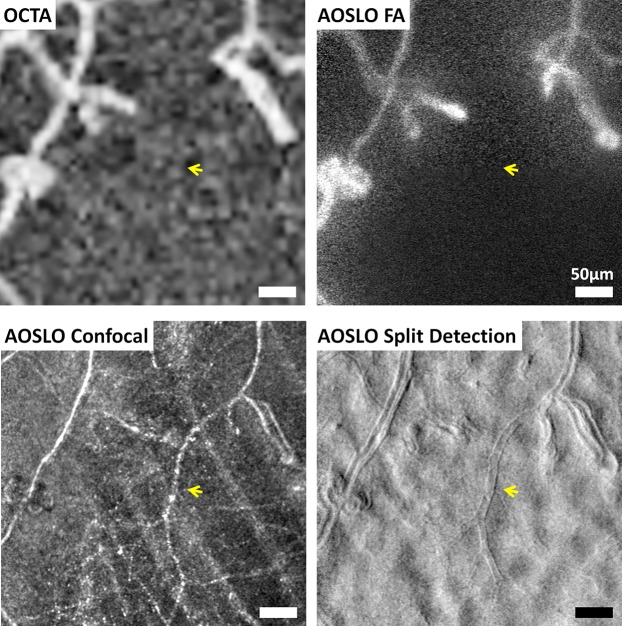
Results: Adaptive optics scanning light ophthalmoscope FA and OCTA showed no statistically significant differences in FAZ perimeter, acircularity index, and vessel densities. Foveal avascular zone area, however, showed a small but statistically significant difference of 1.8% (P = 0.004). Lumen diameter was significantly larger on OCTA (mean difference 5.7 μm, P < 0.001). Microaneurysms, fine structure of vessel loops, leakage, and some vessel segments were visible on AOSLO FA but not OCTA, while blood vessels obscured by leakage were visible only on OCTA.
Conclusions: Optical coherence tomography angiography is comparable to AOSLO FA at imaging the foveal microvasculature except for differences in FAZ area, lumen diameter, and some qualitative features. These results, together with its ease of use, short acquisition time, and avoidance of potentially phototoxic blue light, support OCTA as a tool for monitoring ocular pathology and detecting early disease.
Figures

References
-
- Yu PK,, Balaratnasingam C,, Cringle SJ,, McAllister IL,, Provis J,, Yu DY. Microstructure and network organization of the microvasculature in the human macula. Invest Ophthalmol Vis Sci. 2010. ; 51: 6735–6743. - PubMed
-
- Bek T. Regional morphology and pathophysiology of retinal vascular disease. Prog Retin Eye Res. 2013. ; 36: 247–259. - PubMed
-
- Novotny HR,, Alvis DL. A method of photographing fluorescence in circulating blood in the human retina. Circulation. 1961. ; 24: 82–86. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
