

The Economic and Epidemiological Impact of Focusing Voluntary Medical Male Circumcision for HIV Prevention on Specific Age Groups and Regions in Tanzania
- PMID: 27410384
- PMCID: PMC4943708
- DOI: 10.1371/journal.pone.0153363
The Economic and Epidemiological Impact of Focusing Voluntary Medical Male Circumcision for HIV Prevention on Specific Age Groups and Regions in Tanzania
Abstract
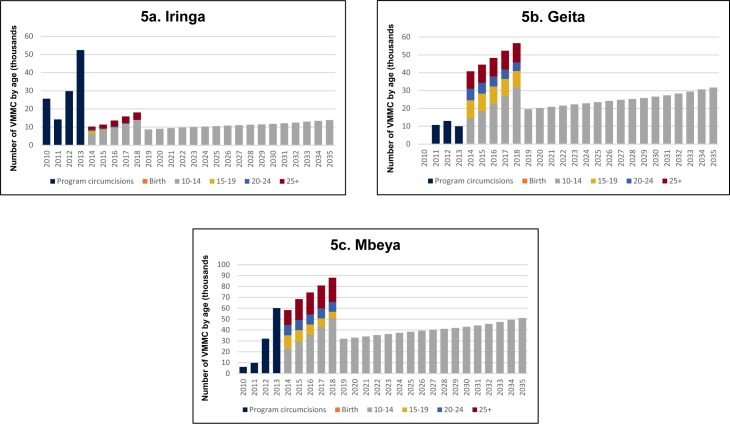
Background: Since its launch in 2010, the Tanzania National Voluntary Medical Male Circumcision (VMMC) Program has focused efforts on males ages 10-34 in 11 priority regions. Implementers have noted that over 70% of VMMC clients are between the ages of 10 and 19, raising questions about whether additional efforts would be required to recruit men age 20 and above. This analysis uses mathematical modeling to examine the economic and epidemiological consequences of scaling up VMMC among specific age groups and priority regions in Tanzania.
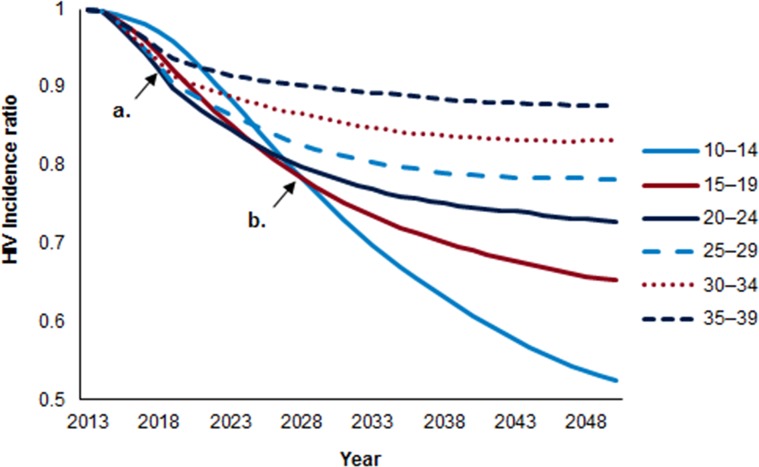
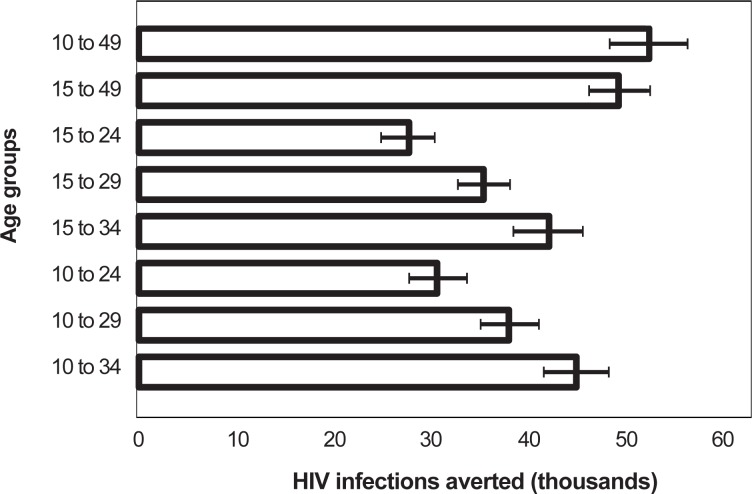
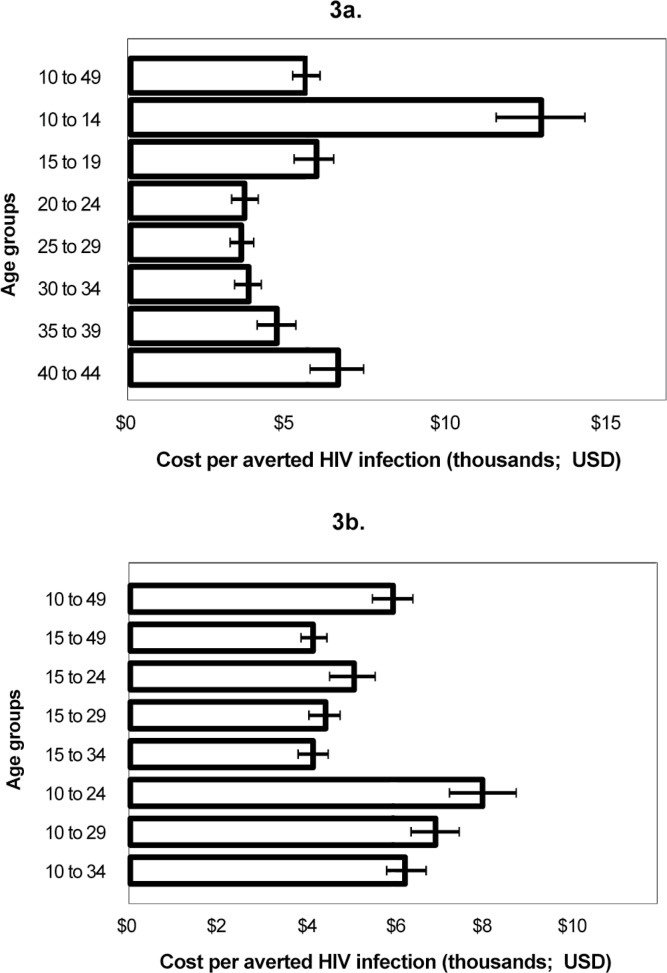
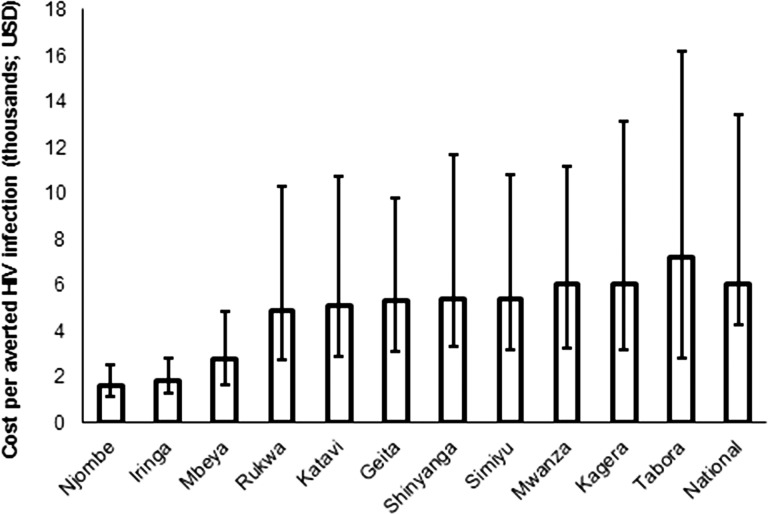
Methods and findings: Analyses were conducted using the Decision Makers' Program Planning Tool Version 2.0 (DMPPT 2.0), a compartmental model implemented in Microsoft Excel 2010. The model was populated with population, mortality, and HIV incidence and prevalence projections from external sources, including outputs from Spectrum/AIDS Impact Module (AIM). A separate DMPPT 2.0 model was created for each of the 11 priority regions. Tanzania can achieve the most immediate impact on HIV incidence by circumcising males ages 20-34. This strategy would also require the fewest VMMCs for each HIV infection averted. Circumcising men ages 10-24 will have the greatest impact on HIV incidence over a 15-year period. The most cost-effective approach (lowest cost per HIV infection averted) targets men ages 15-34. The model shows the VMMC program is cost saving in all 11 priority regions. VMMC program cost-effectiveness varies across regions due to differences in projected HIV incidence, with the most cost-effective programs in Njombe and Iringa.
Conclusions: The DMPPT 2.0 results reinforce Tanzania's current VMMC strategy, providing newfound confidence in investing in circumcising adolescents. Tanzanian policy makers and program implementers will continue to focus scale-up of VMMC on men ages 10-34 years, seeking to maximize program impact and cost-effectiveness while acknowledging trends in demand among the younger and older age groups.
Conflict of interest statement
Figures
References
-
- Cameron DW, Simonsen JN, D'Costa LJ, Ronald AR, Maitha GM, Gakinya MN, et al. Female to male transmission of human immunodeficiency virus type 1: risk factors for seroconversion in men. The Lancet 1989;2(8669):403–7. - PubMed
-
- Bailey RC, Moses S, Parker CB, Agot K, Maclean I, Krieger JN, et al. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. The Lancet 2007;369(9562):643–56. - PubMed
-
- Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S, Nalugoda F, et al. Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. The Lancet 369(9562):p657–66. - PubMed
-
- UNAIDS. New data on male circumcision and HIV prevention: policy and programme implications Montreaux: UNAIDS; 2007.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
