

Inhibition of Midkine Augments Osteoporotic Fracture Healing
- PMID: 27410432
- PMCID: PMC4943649
- DOI: 10.1371/journal.pone.0159278
Inhibition of Midkine Augments Osteoporotic Fracture Healing
Abstract
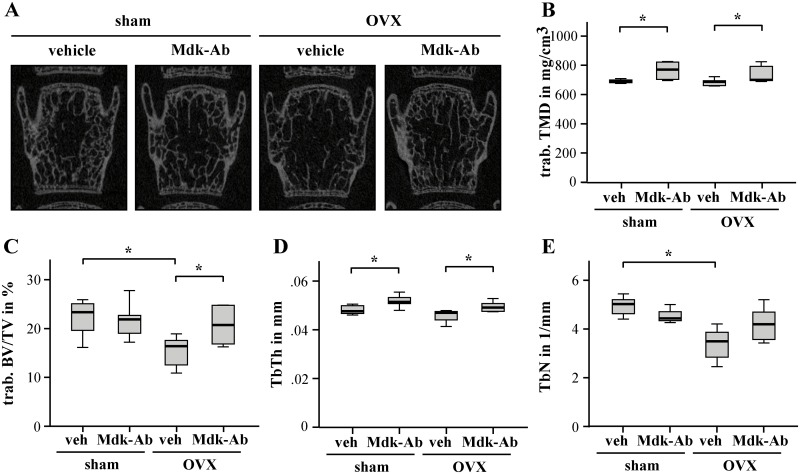
The heparin-binding growth and differentiation factor midkine (Mdk) is proposed to negatively regulate osteoblast activity and bone formation in the adult skeleton. As Mdk-deficient mice were protected from ovariectomy (OVX)-induced bone loss, this factor may also play a role in the pathogenesis of postmenopausal osteoporosis. We have previously demonstrated that Mdk negatively influences bone regeneration during fracture healing. Here, we investigated whether the inhibition of Mdk using an Mdk-antibody (Mdk-Ab) improves compromised bone healing in osteoporotic OVX-mice. Using a standardized femur osteotomy model, we demonstrated that Mdk serum levels were significantly enhanced after fracture in both non-OVX and OVX-mice, however, the increase was considerably greater in osteoporotic mice. Systemic treatment with the Mdk-Ab significantly improved bone healing in osteoporotic mice by increasing bone formation in the fracture callus. On the molecular level, we demonstrated that the OVX-induced reduction of the osteoanabolic beta-catenin signaling in the bony callus was abolished by Mdk-Ab treatment. Furthermore, the injection of the Mdk-Ab increased trabecular bone mass in the skeleton of the osteoporotic mice. These results implicate that antagonizing Mdk may be useful for the therapy of osteoporosis and osteoporotic fracture-healing complications.
Conflict of interest statement
Figures



Similar articles
-
The inflammatory phase of fracture healing is influenced by oestrogen status in mice.Eur J Med Res. 2017 Jul 6;22(1):23. doi: 10.1186/s40001-017-0264-y. Eur J Med Res. 2017. PMID: 28683813 Free PMC article.
-
Antagonizing midkine accelerates fracture healing in mice by enhanced bone formation in the fracture callus.Br J Pharmacol. 2016 Jul;173(14):2237-49. doi: 10.1111/bph.13503. Epub 2016 May 29. Br J Pharmacol. 2016. PMID: 27111560 Free PMC article.
-
Influence of Menopause on Inflammatory Cytokines during Murine and Human Bone Fracture Healing.Int J Mol Sci. 2018 Jul 16;19(7):2070. doi: 10.3390/ijms19072070. Int J Mol Sci. 2018. PMID: 30013010 Free PMC article.
-
Fracture healing in osteoporotic bone.Injury. 2016 Jun;47 Suppl 2:S21-6. doi: 10.1016/S0020-1383(16)47004-X. Injury. 2016. PMID: 27338222 Review.
-
Stem Cell Interventions for Bone Healing: Fractures and Osteoporosis.Curr Stem Cell Res Ther. 2018;13(5):369-377. doi: 10.2174/1574888X13666180410160511. Curr Stem Cell Res Ther. 2018. PMID: 29637866 Review.
Cited by
-
[Influence of hormone or hormone replacement therapy on bone healing].Unfallchirurg. 2019 Jul;122(7):512-517. doi: 10.1007/s00113-019-0677-x. Unfallchirurg. 2019. PMID: 31172230 Review. German.
-
Calcium and vitamin-D deficiency marginally impairs fracture healing but aggravates posttraumatic bone loss in osteoporotic mice.Sci Rep. 2017 Aug 3;7(1):7223. doi: 10.1038/s41598-017-07511-2. Sci Rep. 2017. PMID: 28775273 Free PMC article.
-
The inflammatory phase of fracture healing is influenced by oestrogen status in mice.Eur J Med Res. 2017 Jul 6;22(1):23. doi: 10.1186/s40001-017-0264-y. Eur J Med Res. 2017. PMID: 28683813 Free PMC article.
-
Vasoactive Intestinal Peptide Promotes Fracture Healing in Sympathectomized Mice.Calcif Tissue Int. 2021 Jul;109(1):55-65. doi: 10.1007/s00223-021-00820-9. Epub 2021 May 17. Calcif Tissue Int. 2021. PMID: 33999216
-
Complement receptor C5aR1 on osteoblasts regulates osteoclastogenesis in experimental postmenopausal osteoporosis.Front Endocrinol (Lausanne). 2022 Sep 30;13:1016057. doi: 10.3389/fendo.2022.1016057. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36246887 Free PMC article.
References
-
- Kanis JA. Assessment of osteoporosis at the primary health-care level. World Health Organization Collaborating Centre for Metabolic Bone Diseases. 2007;2007(1):6–166.
-
- Diddle AW, Smith IQ. Postmenopausal osteoporosis: the role of estrogens. South Med J. 1984;77(7):868–74. . - PubMed
-
- Davey DA. Osteoporosis in clinical practice—bone densitometry and fracture risk. S Afr Med J. 1998;88(11):1419–23. . - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
