

Effect of Atomoxetine Treatment on Reading and Phonological Skills in Children with Dyslexia or Attention-Deficit/Hyperactivity Disorder and Comorbid Dyslexia in a Randomized, Placebo-Controlled Trial
- PMID: 27410907
- PMCID: PMC5327054
- DOI: 10.1089/cap.2015.0189
Effect of Atomoxetine Treatment on Reading and Phonological Skills in Children with Dyslexia or Attention-Deficit/Hyperactivity Disorder and Comorbid Dyslexia in a Randomized, Placebo-Controlled Trial
Abstract
Objectives: Evaluated the effects of atomoxetine on the reading abilities of children with dyslexia only or attention-deficit/hyperactivity disorder (ADHD) and comorbid dyslexia.
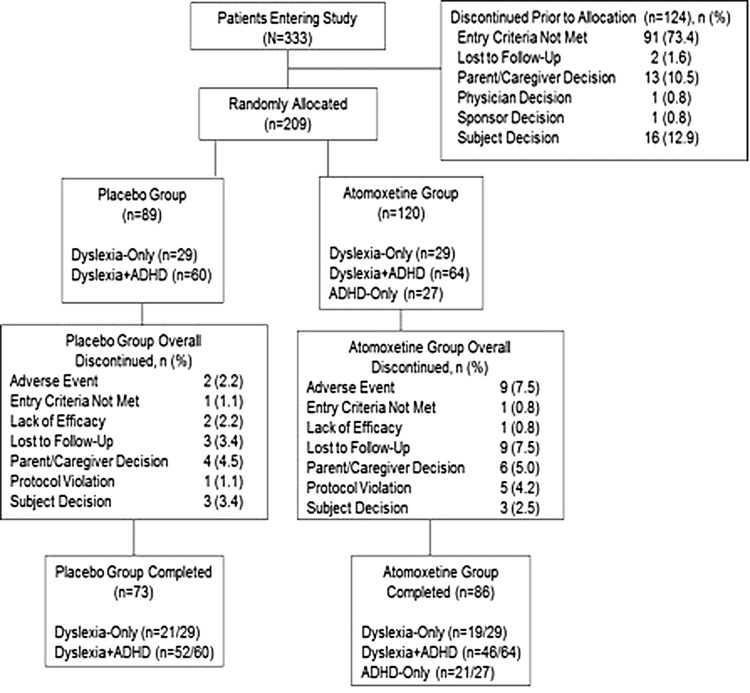
Methods: Children aged 10-16 years (N = 209) met Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) criteria for dyslexia only (n = 58), ADHD and comorbid dyslexia (n = 124), or ADHD only (n = 27) and were of normal intelligence. Patients were treated with atomoxetine (1.0-1.4 mg/kg/day) or placebo in a 16-week, randomized, placebo-controlled, double-blind trial. The dyslexia-only and ADHD and comorbid dyslexia groups were randomized 1:1; the ADHD-only group received atomoxetine in a blinded manner. Reading abilities were measured with the Woodcock Johnson III (WJIII), Comprehensive Test of Phonological Processing (CTOPP), Gray Oral Reading Tests-4, and Test of Word Reading Efficiency.
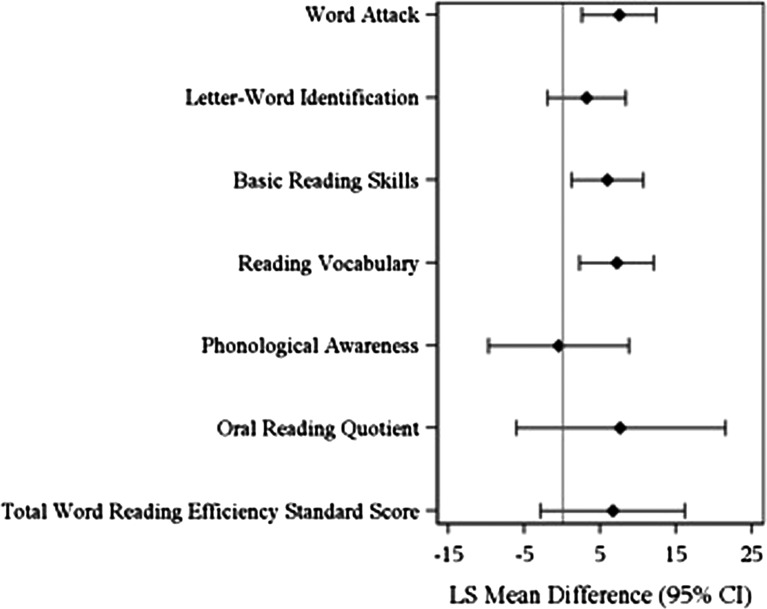
Results: Atomoxetine-treated dyslexia-only patients compared with placebo patients had significantly greater improvement (p < 0.02) with moderate to approaching high effect sizes (ES) on WJIII Word Attack (ES = 0.72), Basic Reading Skills (ES = 0.48), and Reading Vocabulary (ES = 0.73). In the atomoxetine-treated ADHD and comorbid dyslexia group, improvement on the CTOPP Elision measure (ES = 0.50) was significantly greater compared with placebo (p < 0.02). Total, inattentive, and hyperactive/impulsive ADHD symptom reductions were significant in the atomoxetine-treated ADHD and comorbid dyslexia group compared with placebo, and from baseline in the ADHD-only group (p ≤ 0.02). ADHD symptom improvements in the ADHD and comorbid dyslexia group were not correlated with improvements in reading.
Conclusions: Atomoxetine treatment improved reading scores in patients with dyslexia only and ADHD and comorbid dyslexia. Improvements for patients with dyslexia only were in critical components of reading, including decoding and reading vocabulary. For patients with ADHD and comorbid dyslexia, improvements in reading scores were distinct from improvement in ADHD inattention symptoms alone. These data represent the first report of improvements in reading measures following pharmacotherapy treatment in patients with dyslexia only evaluated in a randomized, double-blind trial.
Trial registration: ClinicalTrials.gov NCT00607919.
Keywords: ADHD; atomoxetine; attention; comorbid dyslexia; dyslexia; reading; vocabulary.
Conflict of interest statement
Sally Shaywitz, Bennett Shaywitz—Research support: Eli Lilly and Company.
Linda Wietecha—An employee and minor shareholder of Eli Lilly and Company and/or one of its subsidiaries.
Sharon Wigal—Research support: Addrenex Pharmaceuticals, Inc.; Eli Lilly and Company; Ironshore Pharmaceutical and Development, Inc.; McNeil Consumer Healthcare; NextWave Pharmaceuticals, Inc.; National Institute of Child Health and Human Development; Noven Pharmaceuticals, Inc.; Otsuka America Pharmaceutical, Inc.; Pfizer, Inc.; PsychoGenics; Quintiles, Inc.; Rhodes Pharmaceuticals, L.P.; Shionogi & Co. Ltd.; Shire; Sunovion Pharmaceuticals, Inc.; and Tris Pharma, Inc. Consultant: Eli Lilly and Company; Ironshore Pharmaceutical and Development, Inc.; McNeil Consumer Healthcare; NextWave Pharmaceuticals, Inc; National Institutes of Health; Noven Pharmaceuticals, Inc.; NuTec Systems, Inc.; Pfizer, Inc.; Shire; Sunovion Pharmaceuticals, Inc; Taisho Pharmaceutical Co., Ltd.; and Tris Pharma, Inc. Speaker's bureau: McNeil Consumer Healthcare; Noven Pharmaceuticals, Inc.; Shionogi & Co. Ltd.; and Shire.
Keith McBurnett—Research support: Abbott; Johnson & Johnson; National Institute of Mental Health; Cephalon, Inc.; New River Pharmaceuticals, Inc.; Otsuka America Pharmaceutical, Inc.; Sigma Tau Pharmaceuticals, Inc.; Eli Lilly and Company; McNeil Pharmaceutical; and Shire. Consultant: Lexicor Medical Technology, Eli Lilly and Company, McNeil Pharmaceuticals, and Shire Pharmaceuticals. Honorarium: Received from Lexicon Pharmaceuticals, Inc.
David W. Williams— A full-time employee of inVentiv Health Clinical, LLC, and was a full-time employee of Eli Lilly and Company until October 2010.
William G. Kronenberger—Research support: Eli Lilly and Company, GlaxoSmithKline Plc, Supernus Pharmaceuticals, Inc., Center for Successful Parenting, National Institutes of Health: National Institute on Deafness and Other Communication Disorders and National Library of Medicine, Indiana University, and Indiana Clinical and Translational Sciences Institute. Consultant: Indiana Hemophilia and Thrombosis Center.
Stephen R. Hooper—Research support: Eli Lilly and Company, U.S. Department of Education Institute of Education Sciences, U.S. Department of Health and Human Services: Maternal and Child Health Bureau, National Institutes of Health: Administration on Developmental Disabilities, National Institute on Deafness and Other Communication Disorders, National Institute on Drug Abuse, National Institute of Diabetes and Digestive and Kidney Diseases, and National Institute of Mental Health. Consultant: Eli Lilly and Company.
Figures
Similar articles
-
Atomoxetine-Related Change in Sluggish Cognitive Tempo Is Partially Independent of Change in Attention-Deficit/Hyperactivity Disorder Inattentive Symptoms.J Child Adolesc Psychopharmacol. 2017 Feb;27(1):38-42. doi: 10.1089/cap.2016.0115. Epub 2016 Nov 15. J Child Adolesc Psychopharmacol. 2017. PMID: 27845858 Clinical Trial.
-
Atomoxetine improved attention in children and adolescents with attention-deficit/hyperactivity disorder and dyslexia in a 16 week, acute, randomized, double-blind trial.J Child Adolesc Psychopharmacol. 2013 Nov;23(9):605-13. doi: 10.1089/cap.2013.0054. Epub 2013 Nov 9. J Child Adolesc Psychopharmacol. 2013. PMID: 24206099 Free PMC article. Clinical Trial.
-
Atomoxetine versus placebo in children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder: a double-blind, randomized, multicenter trial in Germany.J Child Adolesc Psychopharmacol. 2011 Apr;21(2):97-110. doi: 10.1089/cap.2009.0111. Epub 2011 Apr 13. J Child Adolesc Psychopharmacol. 2011. PMID: 21488751 Clinical Trial.
-
Atomoxetine for attention deficit hyperactivity disorder in children and adolescents with autism: A systematic review and meta-analysis.Autism Res. 2019 Apr;12(4):542-552. doi: 10.1002/aur.2059. Epub 2019 Jan 17. Autism Res. 2019. PMID: 30653855
-
A systematic review of the use of atomoxetine for management of comorbid anxiety disorders in children and adolescents with attention-deficit hyperactivity disorder.Res Dev Disabil. 2022 Sep;128:104275. doi: 10.1016/j.ridd.2022.104275. Epub 2022 Jun 9. Res Dev Disabil. 2022. PMID: 35691145
Cited by
-
The Effects of ADHD Treatment and Reading Intervention on the Fluency and Comprehension of Children with ADHD and Word Reading Difficulties: A Randomized Clinical Trial.Sci Stud Read. 2020;24(1):72-89. doi: 10.1080/10888438.2019.1640704. Epub 2019 Jul 19. Sci Stud Read. 2020. PMID: 32982141 Free PMC article.
-
Using ADHD Medications to Treat Coexisting ADHD and Reading Disorders: A Systematic Review.Clin Pharmacol Ther. 2018 Oct;104(4):619-637. doi: 10.1002/cpt.1192. Epub 2018 Aug 30. Clin Pharmacol Ther. 2018. PMID: 30053315 Free PMC article.
-
Neural Noise Hypothesis of Developmental Dyslexia.Trends Cogn Sci. 2017 Jun;21(6):434-448. doi: 10.1016/j.tics.2017.03.008. Epub 2017 Apr 8. Trends Cogn Sci. 2017. PMID: 28400089 Free PMC article. Review.
-
Gender-Dependent Changes in Time Production Following Quadrato Motor Training in Dyslexic and Normal Readers.Front Comput Neurosci. 2018 Aug 29;12:71. doi: 10.3389/fncom.2018.00071. eCollection 2018. Front Comput Neurosci. 2018. PMID: 30210326 Free PMC article.
-
The Mechanism, Clinical Efficacy, Safety, and Dosage Regimen of Atomoxetine for ADHD Therapy in Children: A Narrative Review.Front Psychiatry. 2022 Feb 9;12:780921. doi: 10.3389/fpsyt.2021.780921. eCollection 2021. Front Psychiatry. 2022. PMID: 35222104 Free PMC article. Review.
References
-
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. 4th ed., Text Revision. Washington, DC: American Psychological Association; 2000
-
- August GJ, Garfinkel BD: Comorbidity of ADHD and reading disability among clinic-referred children. J Abnorm Child Psychol 18:29–45, 1990 - PubMed
-
- Bental B, Tirosh E: The effects of methylphenidate on word decoding accuracy in boys with attention-deficit/hyperactivity disorder. J Clin Psychopharmacol 28:89–92, 2008 - PubMed
-
- Blackorby J, Wagner M: Longitudinal postschool outcomes of youth with disabilities: Findings from the National Longitudinal Transition Study. Except Child 62:399–413, 1996
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous