

Cost-effectiveness of implantable cardiac devices in patients with systolic heart failure
- PMID: 27411837
- PMCID: PMC5099208
- DOI: 10.1136/heartjnl-2015-308883
Cost-effectiveness of implantable cardiac devices in patients with systolic heart failure
Abstract
Objective: To evaluate the cost-effectiveness of implantable cardioverter defibrillators (ICDs), cardiac resynchronisation therapy pacemakers (CRT-Ps) and combination therapy (CRT-D) in patients with heart failure with reduced ejection fraction based on a range of clinical characteristics.
Methods: Individual patient data from 13 randomised trials were used to inform a decision analytical model. A series of regression equations were used to predict baseline all-cause mortality, hospitalisation rates and health-related quality of life and device-related treatment effects. Clinical variables used in these equations were age, QRS duration, New York Heart Association (NYHA) class, ischaemic aetiology and left bundle branch block (LBBB). A UK National Health Service perspective and a lifetime time horizon were used. Benefits were expressed as quality-adjusted life-years (QALYs). Results were reported for 24 subgroups based on LBBB status, QRS duration and NYHA class.
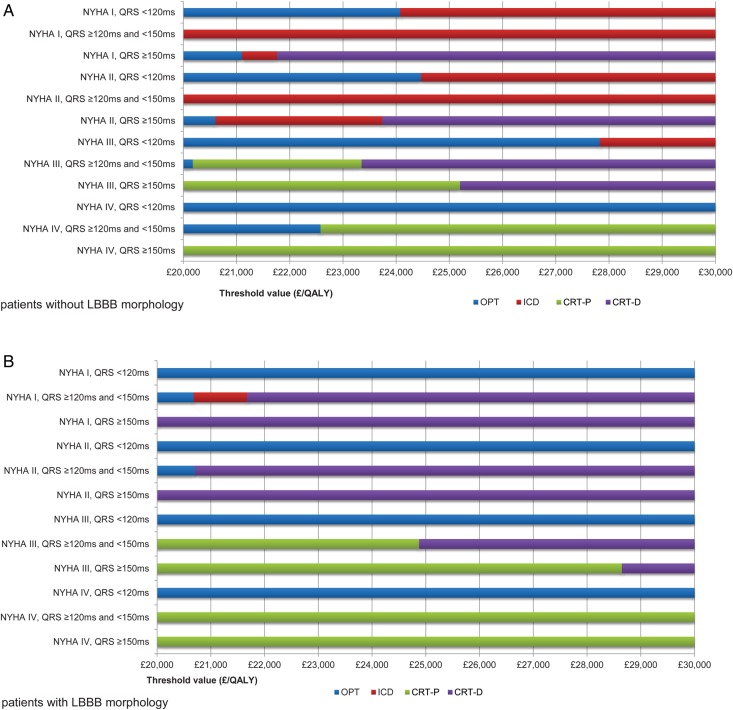
Results: At a threshold of £30 000 per QALY gained, CRT-D was cost-effective in 10 of the 24 subgroups including all LBBB morphology patients with NYHA I/II/III. ICD is cost-effective for all non-NYHA IV patients with QRS duration <120 ms and for NYHA I/II non-LBBB morphology patients with QRS duration between 120 ms and 149 ms. CRT-P was also cost-effective in all NYHA III/IV patients with QRS duration >120 ms. Device therapy is cost-effective in most patient groups with LBBB at a threshold of £20 000 per QALY gained. Results were robust to altering key model parameters.
Conclusions: At a threshold of £30 000 per QALY gained, CRT-D is cost-effective in a far wider group than previously recommended in the UK. In some subgroups ICD and CRT-P remain the cost-effective choice.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
BW, SM, and NH were employees of ICON during the period of this work. MS is a consultant to ICON. and received payment for his involvement in this work. MRC provides consultancy advice to Medtronic, Boston Scientific and St. Jude Medical and has had research grants from Medtronic. CJP has received research funding and travel grants to attend scientific meetings and has provided consultancy advice to Medtronic, Boston Scientific and St. Jude Medical. HK has provided consultancy advice and has received research funding from Boston Scientific. WA has received consulting fees from St. Jude Medical and Biotronik.
Figures
References
-
- Hunt SA, Abraham WT, Chin MH, et al. . ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation 2005;112:e154–235. 10.1161/CIRCULATIONAHA.105.167586 - DOI - PubMed
-
- Jessup M, Abraham WT, Casey DE, et al. . 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation 2009;119:1977–2016. 10.1161/CIRCULATIONAHA.109.192064 - DOI - PubMed
-
- McMurray JJ, Adamopoulos S, Anker SD, et al. . ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2012;14:803–69. 10.1093/eurjhf/hfs105 - DOI - PubMed
-
- Linde C, Mealing S, Hawkins N, et al. . Cost-effectiveness of cardiac resynchronization therapy in patients with asymptomatic to mild heart failure: insights from the European cohort of the REVERSE (Resynchronization Reverses remodeling in Systolic Left Ventricular Dysfunction). Eur Heart J 2011;32:1631–9. 10.1093/eurheartj/ehq408 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials