

Affective disturbance in rheumatoid arthritis: psychological and disease-related pathways
- PMID: 27411910
- PMCID: PMC5449457
- DOI: 10.1038/nrrheum.2016.112
Affective disturbance in rheumatoid arthritis: psychological and disease-related pathways
Abstract
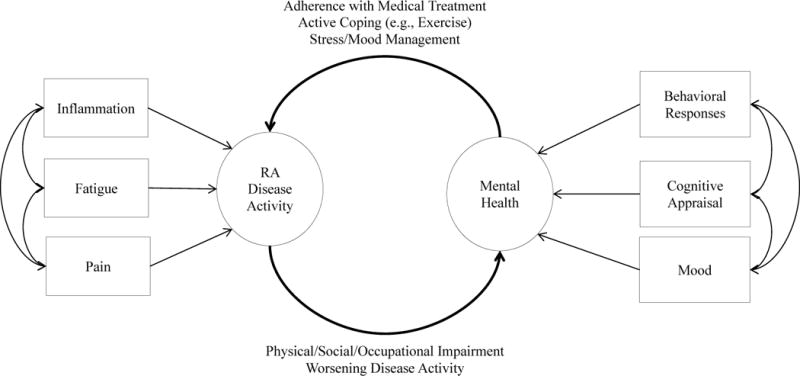
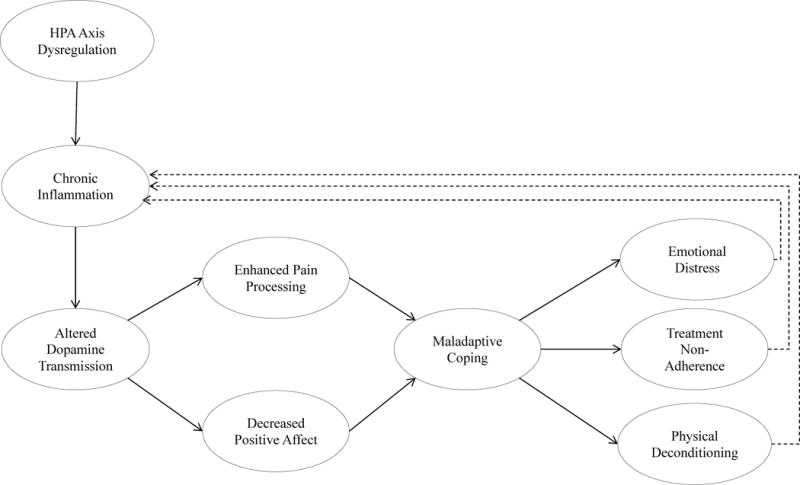
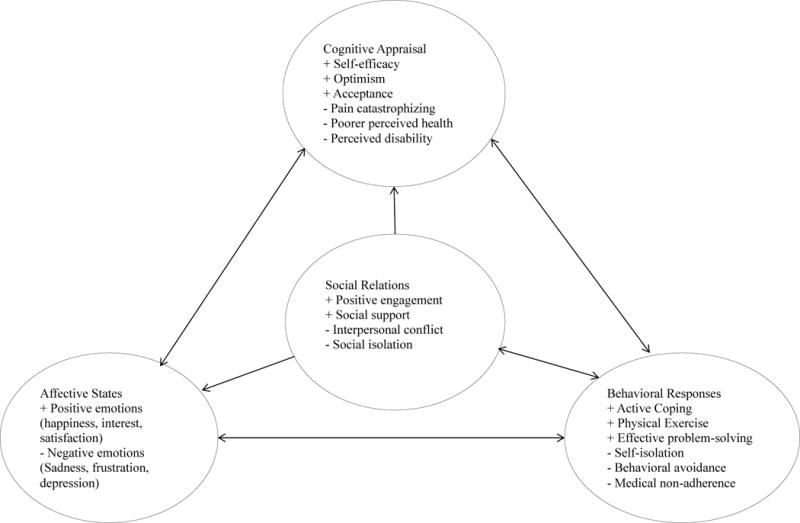
In addition to recurrent pain, fatigue, and increased rates of physical disability, individuals with rheumatoid arthritis (RA) have an increased prevalence of some mental health disorders, particularly those involving affective or mood disturbances. This narrative Review provides an overview of mental health comorbidities in RA, and discusses how these comorbidities interact with disease processes, including dysregulation of inflammatory responses, prolonged difficulties with pain and fatigue, and the development of cognitive and behavioural responses that could exacerbate the physical and psychological difficulties associated with RA. This article describes how the social context of individuals with RA affects both their coping strategies and their psychological responses to the disease, and can also impair responses to treatment through disruption of patient-physician relationships and treatment adherence. Evidence from the literature on chronic pain suggests that the resulting alterations in neural pathways of reward processing could yield new insights into the connections between disease processes in RA and psychological distress. Finally, the role of psychological interventions in the effective and comprehensive treatment of RA is discussed.
Conflict of interest statement
The authors declare no competing interests
Figures
References
-
- Sokka T, Krishnan E, Häkkinen A, Hannonen P. Functional disability in rheumatoid arthritis patients compared with a community population in Finland. Arthritis Rheum. 2003;48:59–63. - PubMed
-
- van’t Land H, et al. The association between arthritis and psychiatric disorders; results from a longitudinal population-based study. J Psychosom Res. 2010;68:187–193. - PubMed
-
- Rupp I, et al. Poor and good health outcomes in rheumatoid arthritis: the role of comorbidity. J Rheumatol. 2006;33:1488–1495. - PubMed
-
- Löwe B, et al. Psychiatric comorbidity and work disability in patients with inflammatory rheumatic diseases. Psychosom Med. 2004;66:395–402. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
