

The effect of non-small cell lung cancer histology on survival as measured by the graded prognostic assessment in patients with brain metastases treated by hypofractionated stereotactic radiotherapy
- PMID: 27411944
- PMCID: PMC4944239
- DOI: 10.1186/s13014-016-0667-x
The effect of non-small cell lung cancer histology on survival as measured by the graded prognostic assessment in patients with brain metastases treated by hypofractionated stereotactic radiotherapy
Abstract
Background: The purpose of this study was to investigate the impact of histology on survival stratified by the Graded Prognostic Assessment (GPA) for non-small cell lung cancer (NSCLC) in a group of selected patients treated recently.
Methods: A total of 171 NSCLC patients with brain metastases treated by hypofractionated stereotactic radiotherapy with or without whole-brain radiotherapy between 2001 and 2011 were included. The GPA score was calculated for each patient. Tumor histologies were categorized into adenocarcinoma (ADCA) and non-ADCA. Median survival time (MST, in months) was calculated using the Kaplan-Meier method. The log-rank test was used to determine statistical differences.
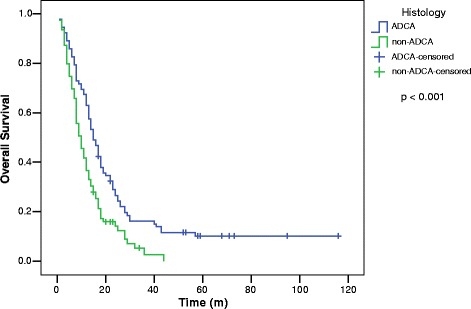
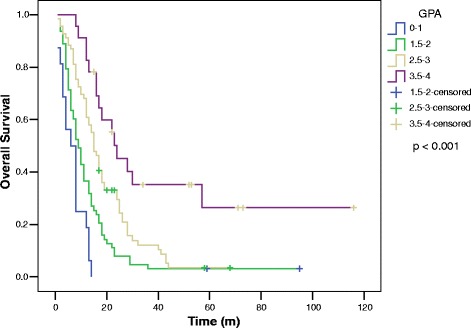
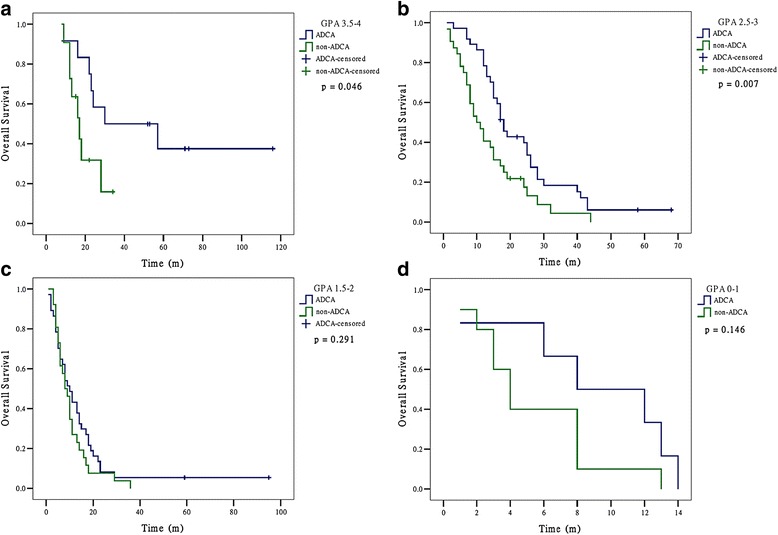
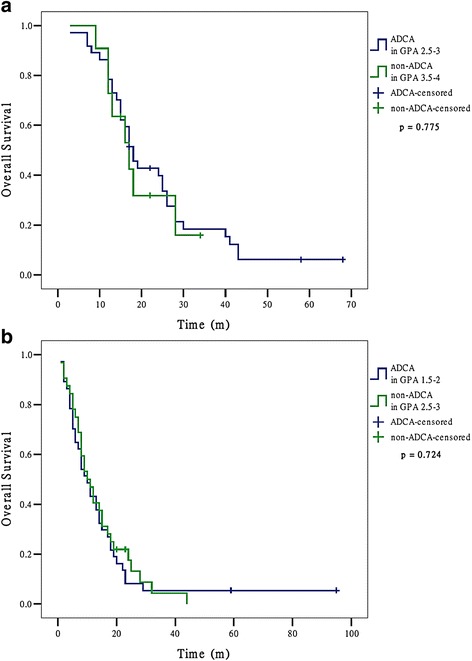
Results: MSTs by histology were: ADCA 15 (n = 92) and non-ADCA 10 (n = 79) (p < 0.001). For all patients, the MSTs by GPA score were: GPA 3.5-4, 24; GPA 2.5-3, 15; GPA 1.5-2, 9 and GPA 0-1, 6 (p < 0.001). The histology of ADCA showed a statistically significant higher MST than non-ADCA for patients with GPA 2.5-4. For GPA 2.5-3, MSTs were: ADCA 18, non-ADCA 10 (p = 0.007); for GPA 3.5-4, MSTs were: ADCA 30, non-ADCA 17 (p = 0.046). For GPA 0-2, MSTs did not differ significantly by histology. For GPA 0-1, MSTs were: ADCA 8, non-ADCA 4 (p = 0.146); GPA 1.5-2, MSTs were: ADCA 10, non-ADCA 8 (p = 0.291). We further found that non-ADCA in upper GPA class (3.5-4) had similar survival with ADCA in lower GPA class (2.5-3) (MSTs were 17 and 18, respectively, p = 0.775). This phenomenon also happened between patients of non-ADCA in upper GPA class (2.5-3) and those of ADCA in lower GPA class (1.5-2) (MSTs were both 10, p = 0.724).
Conclusions: We confirmed that the histology of NSCLC had effect on the GPA in these selected patients treated recently. ADCA showed a statistically significant higher MST than non-ADCA with GPA 2.5-4. The non-ADCA in upper GPA classes (3.5-4 and 2.5-3) had similar survival to ADCA in lower GPA classes (2.5-3 and 1.5-2, respectively). The histology as a new factor should be added to the original GPA for NSCLC.
Keywords: Brain metastases; Graded prognostic assessment; Histology; Hypofractionated stereotactic radiotherapy; Non-small cell lung cancer.
Figures
References
-
- Gaspar L, Scott C, Rotman M, Asbell S, Phillips T, Wasserman T, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys. 1997;37:745–51. doi: 10.1016/S0360-3016(96)00619-0. - DOI - PubMed
-
- Golden DW, Lamborn KR, McDermott MW, Kunwar S, Wara WM, Nakamura JL, et al. Prognostic factors and grading systems for overall survival in patients treated with radiosurgery for brain metastases: variation by primary site. J Neurosurg. 2008;109(Suppl):77–86. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
