

ECG Criteria to Differentiate Between Takotsubo (Stress) Cardiomyopathy and Myocardial Infarction
- PMID: 27412903
- PMCID: PMC4937281
- DOI: 10.1161/JAHA.116.003418
ECG Criteria to Differentiate Between Takotsubo (Stress) Cardiomyopathy and Myocardial Infarction
Abstract
Background: ECG criteria differentiating Takotsubo cardiomyopathy (TTC) from mainly anterior myocardial infarction (MI) have been suggested; however, this was in small patient populations.
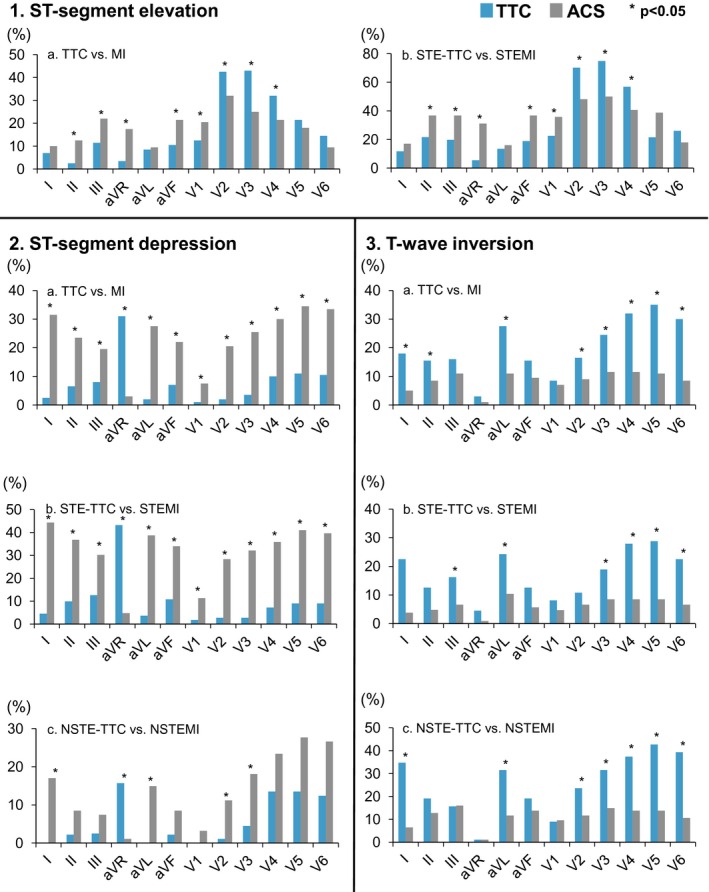
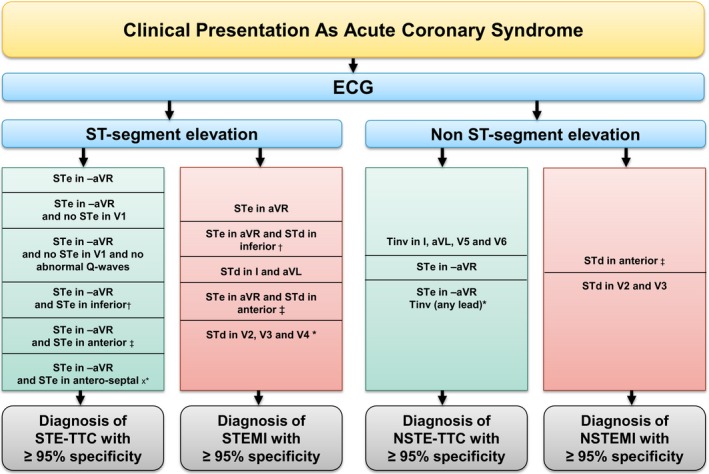
Methods and results: Twelve-lead admission ECGs of consecutive 200 TTC and 200 MI patients were compared in dichotomized groups based on the presence or absence of ST-elevation MI (STEMI versus STE-TTC and non-ST elevation MI versus non ST-elevation-TTC). When comparing STEMI and STE-TTC, ST-elevation in -aVR was characteristic of STE-TTC with a sensitivity/specificity of 43% and 95%, positive predictive value (PPV) 91%, and a negative predictive value (NPV) 62% (P<0.001); when ST-elevation in -aVR is accompanied by ST-elevation in inferior leads, sensitivity/specificity were 14% and 98% (PPV was 89% and NPV 52%) (P=0.001), and 12% and 100% when associated with ST-elevation in anteroseptal leads (PPV 100%, NPV 52%) (P<0.001). On the other hand, STEMI was characterized by ST-elevation in aVR (sensitivity/specificity of 31% and 95% P<0.001, PPV 85% and NPV 59%) and ST-depression in V2-V3-V4 (sensitivity/specificity of 24% and 100% P<0.001, PPV 100% and NPV 76%). When comparing non-ST elevation MI and non ST-elevation-TTC, T-inversion in leads I-aVL-V5-V6 had a sensitivity/specificity of 17% and 97% for non ST-elevation-TTC (PPV 83% and NPV 55%) (P<0.001), and ST-elevation in -aVR with T-inversion in any lead was also specific for non ST-elevation-TTC (sensitivity/specificity of 8% and 100%, PPV 100% and NPV 53%) (P=0.006). In non-ST elevation MI patients, the presence of ST-depression in V2-V3 was specific (sensitivity/specificity of 11% and 99%, PPV 91% and NPV 51%) (P=0.01).
Conclusions: ECG on admission can differentiate between TTC and acute MI, with high specificity and positive predictive value.
Clinical trial registration: URL: https://www.clinicaltrials.gov/. Unique identifier: NCT01947621.
Keywords: Takotsubo cardiomyopathy; differential diagnosis; electrocardiogram; myocardial infarction; stress‐induced cardiomyopathy.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, Cammann VL, Sarcon A, Geyer V, Neumann CA, Seifert B, Hellermann J, Schwyzer M, Eisenhardt K, Jenewein J, Franke J, Katus HA, Burgdorf C, Schunkert H, Moeller C, Thiele H, Bauersachs J, Tschope C, Schultheiss HP, Laney CA, Rajan L, Michels G, Pfister R, Ukena C, Bohm M, Erbel R, Cuneo A, Kuck KH, Jacobshagen C, Hasenfuss G, Karakas M, Koenig W, Rottbauer W, Said SM, Braun‐Dullaeus RC, Cuculi F, Banning A, Fischer TA, Vasankari T, Airaksinen KE, Fijalkowski M, Rynkiewicz A, Pawlak M, Opolski G, Dworakowski R, MacCarthy P, Kaiser C, Osswald S, Galiuto L, Crea F, Dichtl W, Franz WM, Empen K, Felix SB, Delmas C, Lairez O, Erne P, Bax JJ, Ford I, Ruschitzka F, Prasad A, Luscher TF. Clinical features and outcomes of Takotsubo (stress) cardiomyopathy. N Engl J Med. 2015;373:929–938. - PubMed
-
- Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, Rihal CS. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST‐segment elevation myocardial infarction. Ann Intern Med. 2004;141:858–865. - PubMed
-
- Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or Takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006;27:1523–1529. - PubMed
-
- Pilgrim TM, Wyss TR. Takotsubo cardiomyopathy or transient left ventricular apical ballooning syndrome: a systematic review. Int J Cardiol. 2008;124:283–292. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
