

Effectiveness and Safety of Dabigatran, Rivaroxaban, and Apixaban Versus Warfarin in Nonvalvular Atrial Fibrillation
- PMID: 27412905
- PMCID: PMC4937291
- DOI: 10.1161/JAHA.116.003725
Effectiveness and Safety of Dabigatran, Rivaroxaban, and Apixaban Versus Warfarin in Nonvalvular Atrial Fibrillation
Abstract
Background: The introduction of non-vitamin K antagonist oral anticoagulants has been a major advance for stroke prevention in atrial fibrillation; however, outcomes achieved in clinical trials may not translate to routine practice. We aimed to evaluate the effectiveness and safety of dabigatran, rivaroxaban, and apixaban by comparing each agent with warfarin.
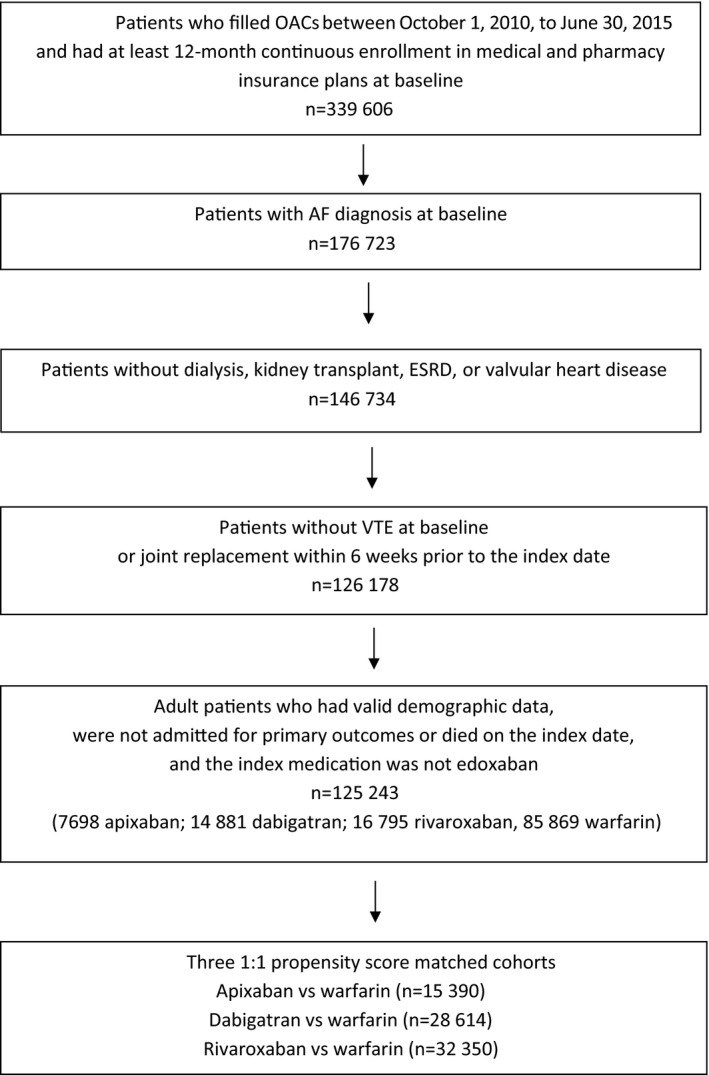
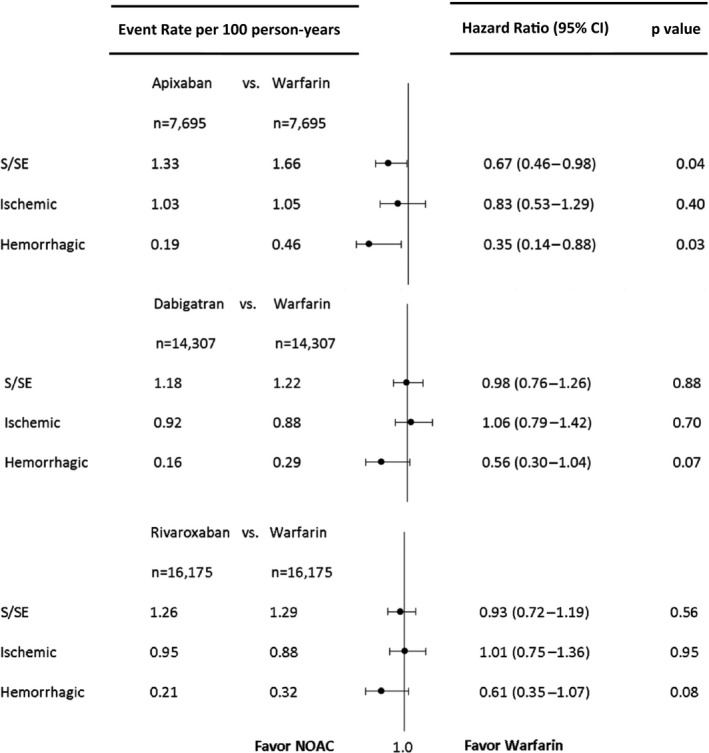
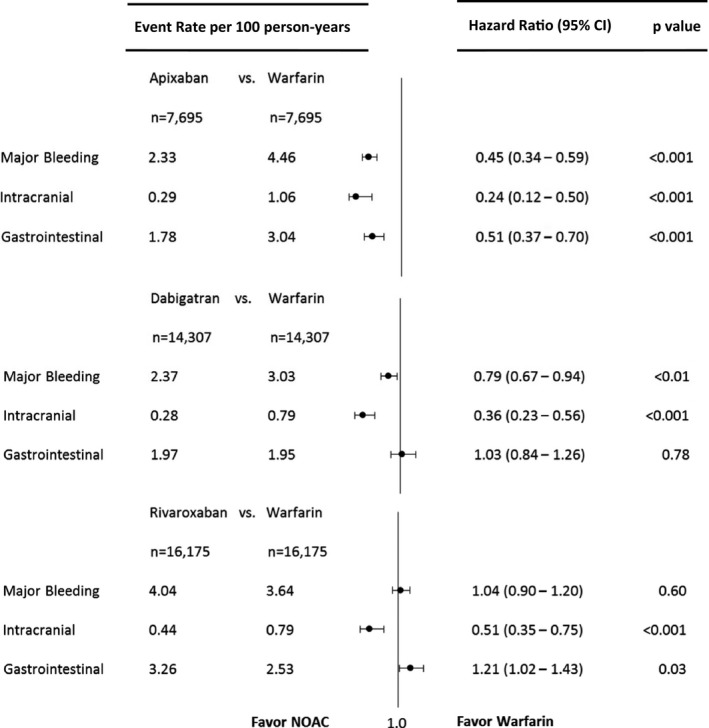
Methods and results: Using a large US insurance database, we identified privately insured and Medicare Advantage patients with nonvalvular atrial fibrillation who were users of apixaban, dabigatran, rivaroxaban, or warfarin between October 1, 2010, and June 30, 2015. We created 3 matched cohorts using 1:1 propensity score matching: apixaban versus warfarin (n=15 390), dabigatran versus warfarin (n=28 614), and rivaroxaban versus warfarin (n=32 350). Using Cox proportional hazards regression, we found that for stroke or systemic embolism, apixaban was associated with lower risk (hazard ratio [HR] 0.67, 95% CI 0.46-0.98, P=0.04), but dabigatran and rivaroxaban were associated with a similar risk (dabigatran: HR 0.98, 95% CI 0.76-1.26, P=0.98; rivaroxaban: HR 0.93, 95% CI 0.72-1.19, P=0.56). For major bleeding, apixaban and dabigatran were associated with lower risk (apixaban: HR 0.45, 95% CI 0.34-0.59, P<0.001; dabigatran: HR 0.79, 95% CI 0.67-0.94, P<0.01), and rivaroxaban was associated with a similar risk (HR 1.04, 95% CI 0.90-1.20], P=0.60). All non-vitamin K antagonist oral anticoagulants were associated with a lower risk of intracranial bleeding.
Conclusions: In patients with nonvalvular atrial fibrillation, apixaban was associated with lower risks of both stroke and major bleeding, dabigatran was associated with similar risk of stroke but lower risk of major bleeding, and rivaroxaban was associated with similar risks of both stroke and major bleeding in comparison to warfarin.
Keywords: atrial fibrillation; bleeding; non–vitamin K antagonist oral anticoagulants; stroke; warfarin.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Lloyd‐Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, Vasan RS, D'Agostino RB, Massaro JM, Beiser A, Wolf PA. Lifetime risk for development of atrial fibrillation the Framingham Heart Study. Circulation. 2004;110:1042–1046. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983–988. - PubMed
-
- Stewart S, Hart CL, Hole DJ, McMurray JJ. A population‐based study of the long‐term risks associated with atrial fibrillation: 20‐year follow‐up of the Renfrew/Paisley study. Am J Med. 2002;113:359–364. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta‐analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–867. - PubMed
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64:e1–e76. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
