

Minnesota Resuscitation Consortium's Advanced Perfusion and Reperfusion Cardiac Life Support Strategy for Out-of-Hospital Refractory Ventricular Fibrillation
- PMID: 27412906
- PMCID: PMC4937292
- DOI: 10.1161/JAHA.116.003732
Minnesota Resuscitation Consortium's Advanced Perfusion and Reperfusion Cardiac Life Support Strategy for Out-of-Hospital Refractory Ventricular Fibrillation
Abstract
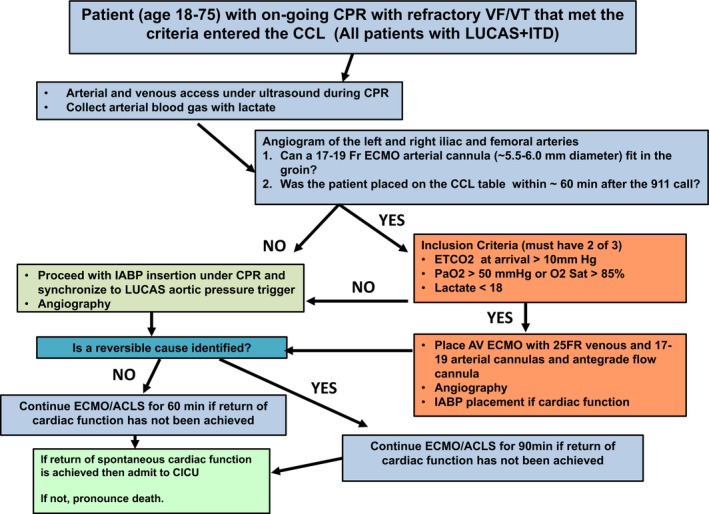
Background: In 2015, the Minnesota Resuscitation Consortium (MRC) implemented an advanced perfusion and reperfusion life support strategy designed to improve outcome for patients with out-of-hospital refractory ventricular fibrillation/ventricular tachycardia (VF/VT). We report the outcomes of the initial 3-month period of operations.
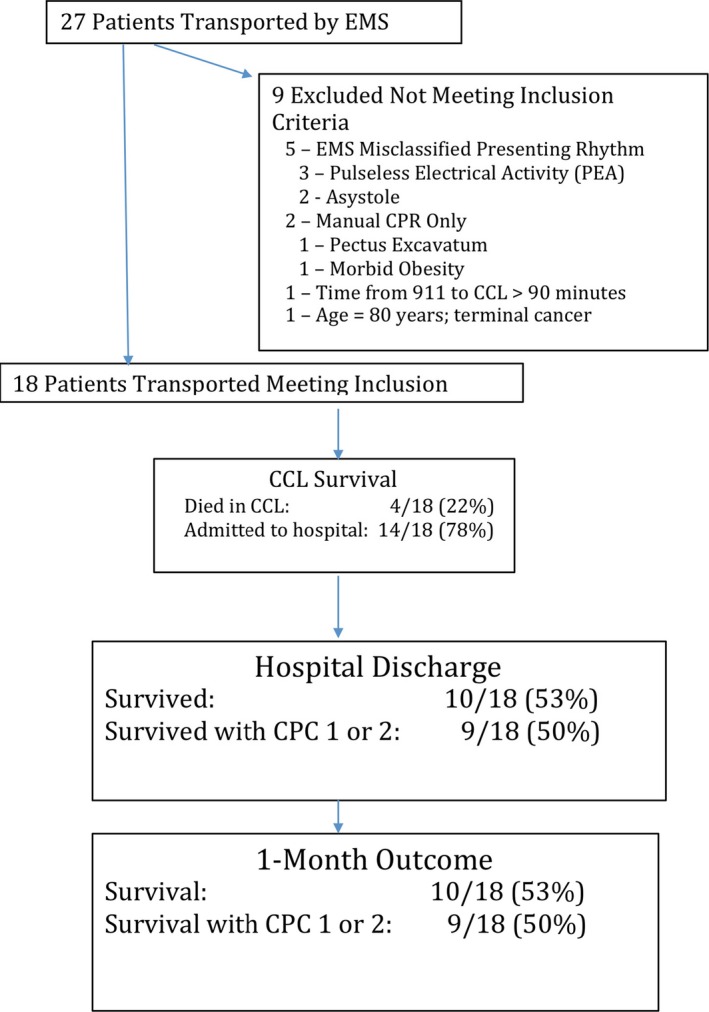
Methods and results: Three emergency medical services systems serving the Minneapolis-St. Paul metro area participated in the protocol. Inclusion criteria included age 18 to 75 years, body habitus accommodating automated Lund University Cardiac Arrest System (LUCAS) cardiopulmonary resuscitation (CPR), and estimated transfer time from the scene to the cardiac catheterization laboratory of ≤30 minutes. Exclusion criteria included known terminal illness, Do Not Resuscitate/Do Not Intubate status, traumatic arrest, and significant bleeding. Refractory VF/VT arrest was defined as failure to achieve sustained return of spontaneous circulation after treatment with 3 direct current shocks and administration of 300 mg of intravenous/intraosseous amiodarone. Patients were transported to the University of Minnesota, where emergent advanced perfusion strategies (extracorporeal membrane oxygenation; ECMO), followed by coronary angiography and primary coronary intervention (PCI), were performed, when appropriate. Over the first 3 months of the protocol, 27 patients were transported with ongoing mechanical CPR. Of these, 18 patients met the inclusion and exclusion criteria. ECMO was placed in 83%. Seventy-eight percent of patients had significant coronary artery disease with a high degree of complexity and 67% received PCI. Seventy-eight percent of patients survived to hospital admission and 55% (10 of 18) survived to hospital discharge, with 50% (9 of 18) achieving good neurological function (cerebral performance categories 1 and 2). No significant ECMO-related complications were encountered.
Conclusions: The MRC refractory VF/VT protocol is feasible and led to a high functionally favorable survival rate with few complications.
Keywords: Extra‐corporeal membrane oxygenation; emergent extracorporeal membrane oxygenation; perfusion; refractory ventricular fibrillation/ventricular tachycardia; resuscitation; ventricular fibrillation.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Aufderheide TP, Frascone RJ, Wayne MA, Mahoney BD, Swor RA, Domeier RM, Olinger ML, Holcomb RG, Tupper DE, Yannopoulos D, Lurie KG. Standard cardiopulmonary resuscitation versus active compression‐decompression cardiopulmonary resuscitation with augmentation of negative intrathoracic pressure for out‐of‐hospital cardiac arrest: a randomised trial. Lancet. 2011;377:301–311. - PMC - PubMed
-
- Aufderheide TP, Nichol G, Rea TD, Brown SP, Leroux BG, Pepe PE, Kudenchuk PJ, Christenson J, Daya MR, Dorian P, Callaway CW, Idris AH, Andrusiek D, Stephens SW, Hostler D, Davis DP, Dunford JV, Pirrallo RG, Stiell IG, Clement CM, Craig A, Van Ottingham L, Schmidt TA, Wang HE, Weisfeldt ML, Ornato JP, Sopko G; Resuscitation Outcomes Consortium I . A trial of an impedance threshold device in out‐of‐hospital cardiac arrest. N Engl J Med. 2011;365:798–806. - PMC - PubMed
-
- Link MS, Berkow LC, Kudenchuk PJ, Halperin HR, Hess EP, Moitra VK, Neumar RW, O'Neil BJ, Paxton JH, Silvers SM, White RD, Yannopoulos D, Donnino MW. Part 7: adult advanced cardiovascular life support: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S444–S464. - PubMed
-
- Spaulding CM, Joly LM, Rosenberg A, Monchi M, Weber SN, Dhainaut JF, Carli P. Immediate coronary angiography in survivors of out‐of‐hospital cardiac arrest. N Engl J Med. 1997;336:1629–1633. - PubMed
-
- Garcia S, Drexel T, Bekwelem W, Raveendran G, Caldwell E, Hodgson L, Wang Q, Adabag S, Mahoney B, Frascone R, Helmer G, Lick C, Conterato M, Baran K, Bart B, Bachour F, Roh S, Panetta C, Stark R, Haugland M, Mooney M, Wesley K, Yannopoulos D. Early access to the cardiac catheterization laboratory for patients resuscitated from cardiac arrest due to a shockable rhythm: the Minnesota Resuscitation Consortium Twin Cities Unified Protocol. J Am Heart Assoc. 2016;5:e002670 doi: 10.1161/JAHA.115.002670. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
