

Diabetes treatments and risk of heart failure, cardiovascular disease, and all cause mortality: cohort study in primary care
- PMID: 27413012
- PMCID: PMC4948032
- DOI: 10.1136/bmj.i3477
Diabetes treatments and risk of heart failure, cardiovascular disease, and all cause mortality: cohort study in primary care
Abstract
Objective: To assess associations between risks of cardiovascular disease, heart failure, and all cause mortality and different diabetes drugs in people with type 2 diabetes, particularly newer agents, including gliptins and thiazolidinediones (glitazones).
Design: Open cohort study.
Setting: 1243 general practices contributing data to the QResearch database in England.
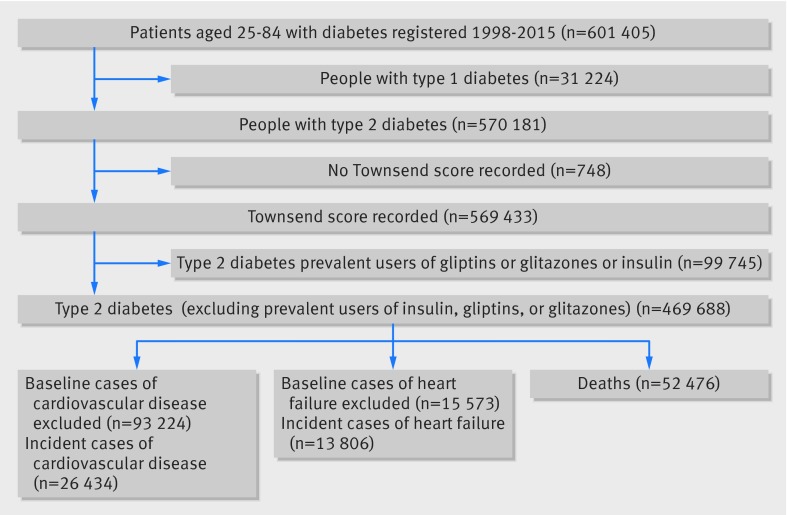
Participants: 469 688 people with type 2 diabetes aged 25-84 years between 1 April 2007 and 31 January 2015.
Exposures: Diabetes drugs (glitazones, gliptins, metformin, sulphonylureas, insulin, other) alone and in combination.
Main outcome measure: First recorded diagnoses of cardiovascular disease, heart failure, and all cause mortality recorded on the patients' primary care, mortality, or hospital record. Cox proportional hazards models were used to estimate hazard ratios for diabetes treatments, adjusting for potential confounders.
Results: During follow-up, 21 308 patients (4.5%) received prescriptions for glitazones and 32 533 (6.9%) received prescriptions for gliptins. Compared with non-use, gliptins were significantly associated with an 18% decreased risk of all cause mortality, a 14% decreased risk of heart failure, and no significant change in risk of cardiovascular disease; corresponding values for glitazones were significantly decreased risks of 23% for all cause mortality, 26% for heart failure, and 25% for cardiovascular disease. Compared with no current treatment, there were no significant associations between monotherapy with gliptins and risk of any complications. Dual treatment with gliptins and metformin was associated with a decreased risk of all three outcomes (reductions of 38% for heart failure, 33% for cardiovascular disease, and 48% for all cause mortality). Triple treatment with metformin, sulphonylureas, and gliptins was associated with a decreased risk of all three outcomes (reductions of 40% for heart failure, 30% for cardiovascular disease, and 51% for all cause mortality). Compared with no current treatment, monotherapy with glitazone was associated with a 50% decreased risk of heart failure, and dual treatment with glitazones and metformin was associated with a decreased risk of all three outcomes (reductions of 50% for heart failure, 54% for cardiovascular disease, and 45% for all cause mortality); dual treatment with glitazones and sulphonylureas was associated with risk reductions of 35% for heart failure and 25% for cardiovascular disease; triple treatment with metformin, sulphonylureas, and glitazones was associated with decreased risks of all three outcomes (reductions of 46% for heart failure, 41% for cardiovascular disease, and 56% for all cause mortality).
Conclusions: There are clinically important differences in risk of cardiovascular disease, heart failure, and all cause mortality between different diabetes drugs alone and in combination. Overall, use of gliptins or glitazones was associated with decreased risks of heart failure, cardiovascular disease, and all cause mortality compared with non-use of these drugs. These results, which do not account for levels of adherence or dosage information and which are subject to confounding by indication, might have implications for prescribing of diabetes drugs.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at

References
-
- Health and Social Care Information Centre. National Diabetes Audit 2012-2013 Report 2 Complications and Mortality. 2014.
-
- Khan SS, Butler J, Gheorghiade M. Management of comorbid diabetes mellitus and worsening heart failure. JAMA 2014;311:2379-80. 10.1001/jama.2014.4115 pmid:24938559. - DOI - PubMed
-
- Scirica BM, Bhatt DL, Braunwald E, et al. SAVOR-TIMI 53 Steering Committee and Investigators. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 2013;369:1317-26. 10.1056/NEJMoa1307684 pmid:23992601. - DOI - PubMed
-
- Home PD, Pocock SJ, Beck-Nielsen H, et al. RECORD Study Team. Rosiglitazone evaluated for cardiovascular outcomes in oral agent combination therapy for type 2 diabetes (RECORD): a multicentre, randomised, open-label trial. Lancet 2009;373:2125-35. 10.1016/S0140-6736(09)60953-3 pmid:19501900. - DOI - PubMed
-
- Tzoulaki I, Molokhia M, Curcin V, Little MP, Millett CJ, Ng A, et alRisk of cardiovascular disease and all cause mortality among patients with type 2 diabetes prescribed oral antidiabetes drugs: retrospective cohort study using UK general practice research database. BMJ 2009;339:b4731. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous