

Obesity Is Associated With Progression of Atherosclerosis During Statin Treatment
- PMID: 27413040
- PMCID: PMC5015399
- DOI: 10.1161/JAHA.116.003621
Obesity Is Associated With Progression of Atherosclerosis During Statin Treatment
Abstract
Background: This study aimed to determine the relationship of statin therapy and cardiovascular risk factors to changes in atherosclerosis in the carotid artery.
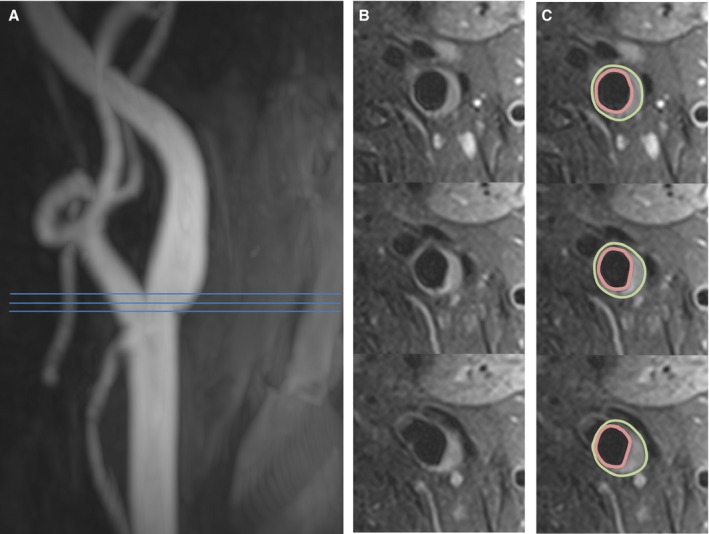
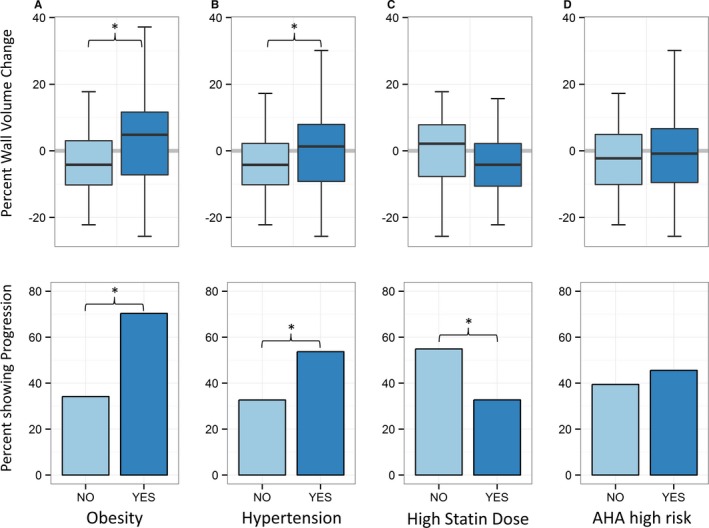
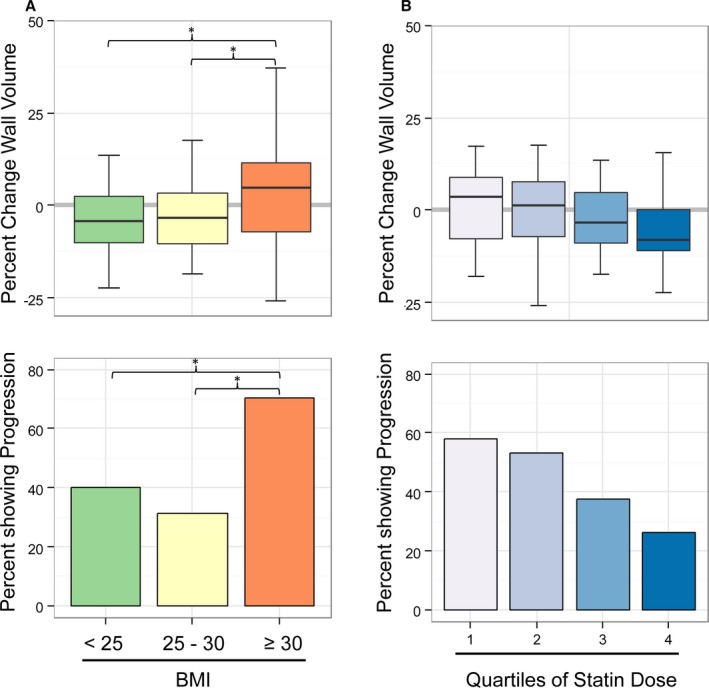
Methods and results: Carotid magnetic resonance imaging was used to evaluate 106 hyperlipidemic participants at baseline and after 12 months of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor (statin) treatment. Multivariable logistic regression was used to determine factors associated with progression (change in carotid wall volume >0) or regression (change ≤0) of carotid atherosclerosis. Computed tomography coronary calcium scores were obtained at baseline for all participants. The median age was 65 years (interquartile range 60-69 years), and 63% of the participants were male. Body mass index >30, elevated C-reactive protein, and hypertension were associated with increased carotid wall volume (obesity: odds ratio for progression 4.6, 95% CI 1.8-12.4, P<0.01; C-reactive protein: odds ratio for progression 2.56, 95% CI 1.17-5.73, P=0.02; hypertension: odds ratio 2.4, 95% CI 1.1-5.3, P<0.05). Higher statin dose was associated with regression of carotid wall volume (P<0.05). In multivariable analysis, obesity remained associated with progression (P<0.01), whereas statin use remained associated with regression (P<0.05). Change in atheroma volume in obese participants was +4.8% versus -4.2% in nonobese participants (P<0.05) despite greater low-density lipoprotein cholesterol reduction in obese participants.
Conclusions: In a population with hyperlipidemia, obese patients showed atheroma progression despite optimized statin therapy.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT01212900.
Keywords: carotid artery; carotid magnetic resonance imaging; obesity.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures

References
-
- Kajinami K, Akao H, Polisecki E, Schaefer EJ. Pharmacogenomics of statin responsiveness. Am J Cardiol. 2005;96:65K–70K; discussion 34K‐35K. - PubMed
-
- Kataoka Y, St John J, Wolski K, Uno K, Puri R, Tuzcu EM, Nissen SE, Nicholls SJ. Atheroma progression in hyporesponders to statin therapy. Arterioscler Thromb Vasc Biol. 2015;35:990–995. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
