

Evaluation of the Safety and Effectiveness of Intense Pulsed Light in the Treatment of Meibomian Gland Dysfunction
- PMID: 27413540
- PMCID: PMC4931092
- DOI: 10.1155/2016/1910694
Evaluation of the Safety and Effectiveness of Intense Pulsed Light in the Treatment of Meibomian Gland Dysfunction
Abstract
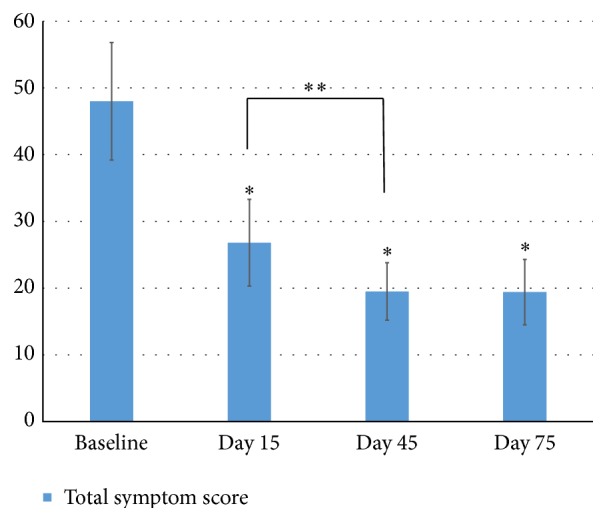
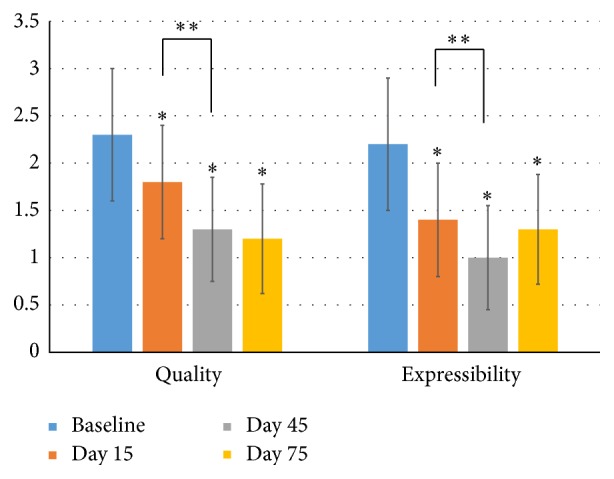
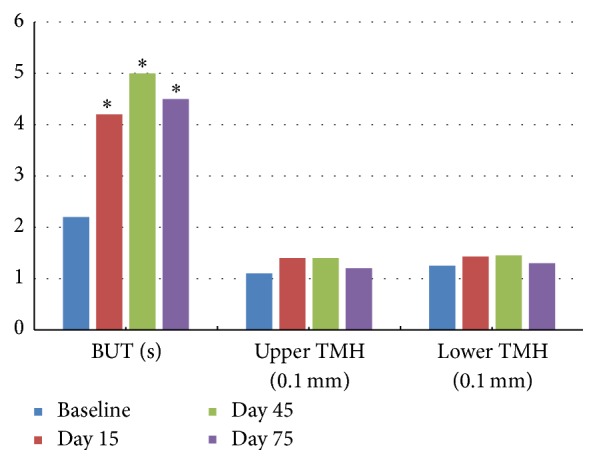
Purpose. This study aims to explore the safety and efficacy of a novel treatment-intense pulsed light (IPL) in MGD eyes. Methods. This study is a prospective and open label study. Forty eyes of 40 MGD patients were recruited in the study and received 4 consecutive IPL treatments on day 1, day 15, day 45, and day 75. Ten ocular surface symptoms were evaluated with a subjective face score at every visit. Best spectacle corrected visual acuity, intraocular pressure (IOP), conjunctival injection, upper and lower tear meniscus height (TMH), tear break-up time (TBUT), corneal staining, lid margin and meibomian gland assessments, and meibography were also recorded at every visit, as well as the adverse effects on the eye and ocular surface. Results. Significant improvements were observed in single and total ocular surface symptom scores, TBUT, and conjunctival injection at all the visits after the initial IPL treatment (P < 0.05). Compared to baseline, the signs of eyelid margin, meibomian gland secretion quality, and expressibility were significantly improved at every visit after treatments. There was no regional and systemic threat observed in any patient. Conclusion. Intense pulsed light (IPL) therapy is a safe and efficient treatment in relieving symptoms and signs of MGD eyes.
Figures
References
-
- Schaumberg D. A., Nichols J. J., Papas E. B., Tong L., Uchino M., Nichols K. K. The international workshop on meibomian gland dysfunction: report of the subcommittee on the epidemiology of, and associated risk factors for, MGD. Investigative Ophthalmology & Visual Science. 2011;52(4):1994–2005. doi: 10.1167/iovs.10-6997e. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
