

Changes in Hepatic Venous Pressure Gradient Induced by Physical Exercise in Cirrhosis: Results of a Pilot Randomized Open Clinical Trial
- PMID: 27415618
- PMCID: PMC5543482
- DOI: 10.1038/ctg.2016.38
Changes in Hepatic Venous Pressure Gradient Induced by Physical Exercise in Cirrhosis: Results of a Pilot Randomized Open Clinical Trial
Abstract
Objectives: Exercise has been scarcely studied in patients with cirrhosis, and prior evidence showed hepatic venous pressure gradient (HVPG) to be increased in response to exercise. The aim of this study was to investigate the effects of a supervised physical exercise program (PEP) in patients with cirrhosis.
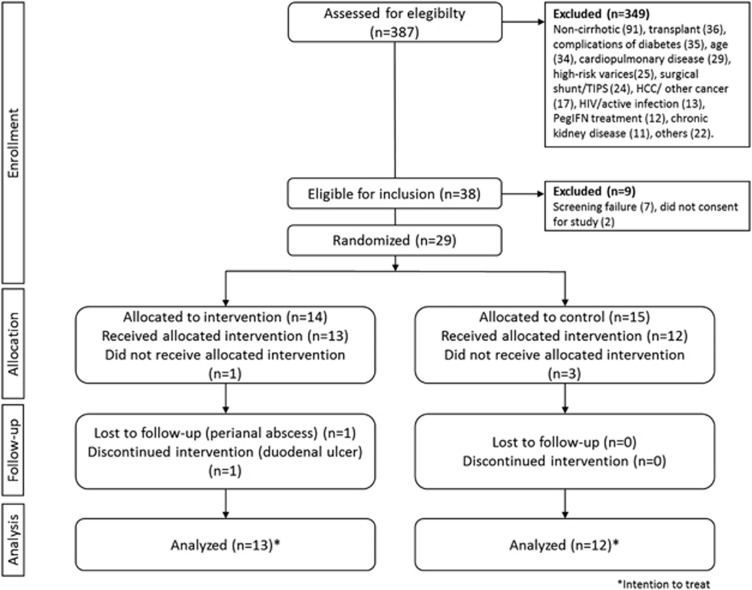
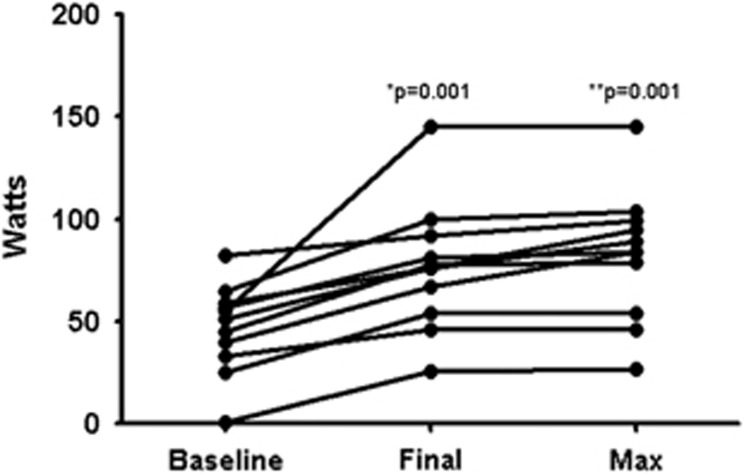
Methods: In an open-label, pilot clinical trial, patients with cirrhosis were randomized to PEP (cycloergometry/kinesiotherapy plus nutritional therapy, n=14) or control (nutritional therapy, n=15); for 14 weeks. Primary outcomes were: the effect of PEP in HVPG, and quality of life (chronic liver disease questionnaire, CLDQ). As secondary outcomes we investigated changes in physical fitness (cardiopulmonary exercise testing), nutritional status (phase angle-bioelectrical impedance), ammonia levels, and safety.
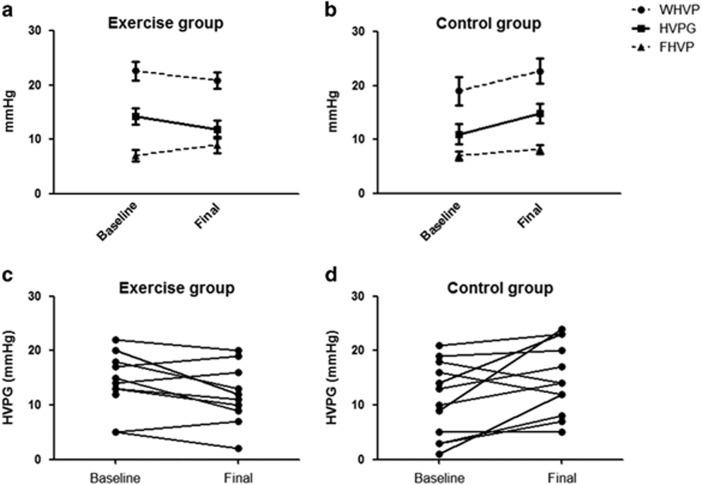
Results: Twenty-two patients completed the study (11 each). HVPG decreased in subjects allocated to PEP (-2.5 mm Hg (interquartile range: -5.25 to 2); P=0.05), and increased in controls (4 mm Hg (0-5); P=0.039), with a significant between-groups difference (P=0.009). No major changes were noted in CLDQ in both groups. There was significant improvement in ventilatory efficiency (VE/VCO2) in PEP group (-1.9 (-3.12 to -0.1); P=0.033), but not in controls (-0.4 (-5.7 to 1.4); P=0.467). Phase angle improvement and a less-pronounced exercise-induced hyperammonemia were noted only in PEP group. No episodes of variceal bleeding or hepatic encephalopathy were observed.
Conclusions: A supervised PEP in patients with cirrhosis decreases the HVPG and improves nutritional status with no changes in quality of life. Further studies evaluating physical training in cirrhosis are eagerly awaited in order to better define the benefits of sustained exercise. ClinicalTrials.gov:NCT00517738.
Conflict of interest statement
Figures
References
-
- Orozco LJ, Buchleitner AM, Gimenez-Perez G et al. Exercise or exercise and diet for preventing type 2 diabetes mellitus. Cochrane Database Syst Rev 2008: CD003054. - PubMed
-
- Wen CP, Wai JP, Tsai MK et al. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet 2011; 378: 1244–1253. - PubMed
-
- Eckel RH, Jakicic JM, Ard JD et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 63: 2960–2984. - PubMed
-
- Garber CE, Blissmer B, Deschenes MR et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 2011; 43: 1334–1359. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
