

Morphological and molecular features of astroblastoma, including BRAFV600E mutations, suggest an ontological relationship to other cortical-based gliomas of children and young adults
- PMID: 27416954
- PMCID: PMC5193018
- DOI: 10.1093/neuonc/now118
Morphological and molecular features of astroblastoma, including BRAFV600E mutations, suggest an ontological relationship to other cortical-based gliomas of children and young adults
Abstract
Background: Astroblastomas (ABs) are rare glial tumors showing overlapping features with astrocytomas, ependymomas, and sometimes other glial neoplasms, and may be challenging to diagnose.
Methods: We examined clinical, histopathological, and molecular features in 28 archival formalin-fixed, paraffin-embedded AB cases and performed survival analyses using Cox proportional hazards and Kaplan-Meier methods.
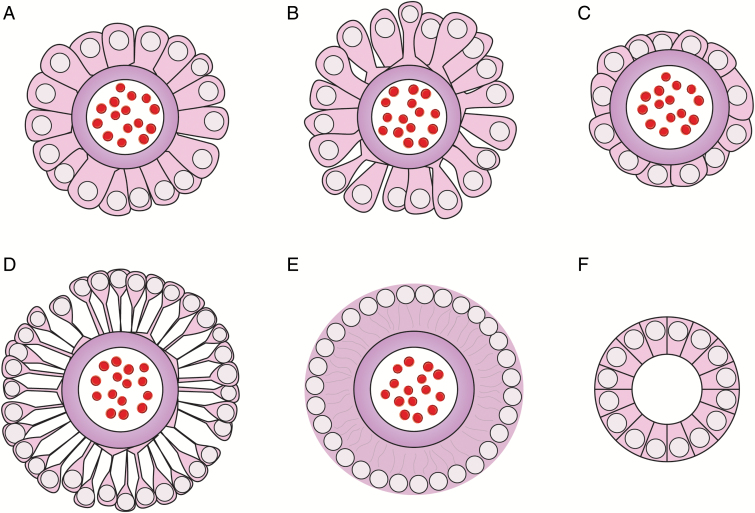
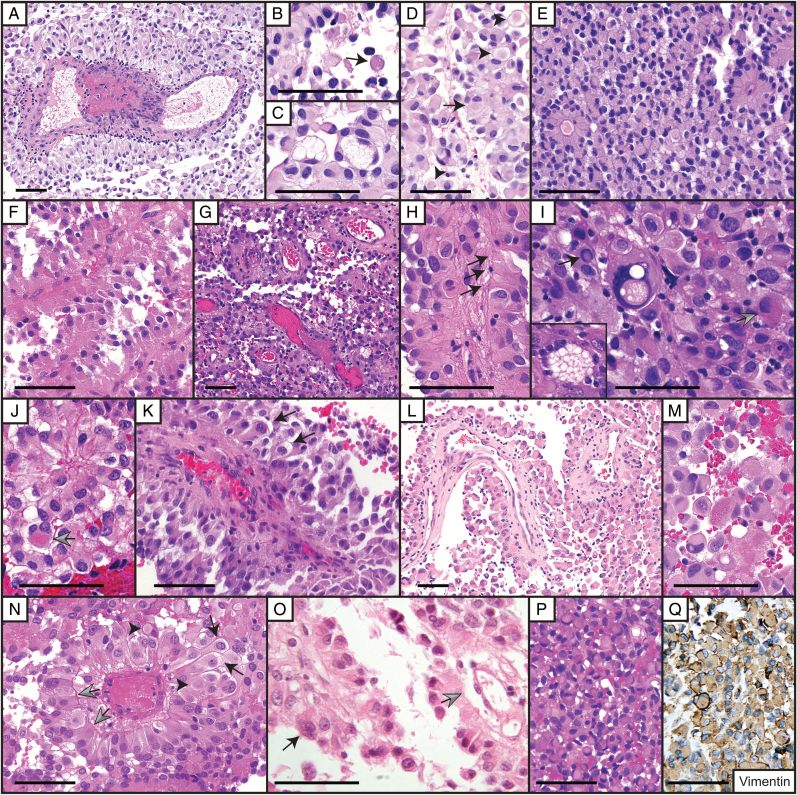
Results: Unlike ependymomas and angiocentric gliomas, ABs demonstrate abundant distinctive astroblastic pseudorosettes and are usually Olig2 immunopositive. They also frequently exhibit rhabdoid cells, multinucleated cells, and eosinophilic granular material. They retain immunoreactivity to alpha thalassemia/mental retardation syndrome X-linked, are immunonegative to isocitrate dehydrogenase-1 R132H mutation, and only occasionally show MGMT promoter hypermethylation differentiating them from many diffuse gliomas. Like pleomorphic xanthoastrocytoma, ganglioglioma, supratentorial pilocytic astrocytoma, and other predominantly cortical-based glial tumors, ABs often harbor the BRAFV600E mutation, present in 38% of cases tested (n = 21), further distinguishing those tumors from ependymomas and angiocentric gliomas. Factors correlating with longer patient survival included age less than 30 years, female gender, absent BRAFV600E , and mitotic index less than 5 mitoses/10 high-power fields; however, only the latter was significant by Cox and Kaplan-Meier analyses (n = 24; P = .024 and .012, respectively). This mitotic cutoff is therefore currently the best criterion to stratify tumors into low-grade ABs and higher-grade anaplastic ABs.
Conclusions: In addition to their own characteristic histological features, ABs share some molecular and histological findings with other, possibly ontologically related, cortical-based gliomas of mostly children and young adults. Importantly, the presence of BRAFV600E mutations in a subset of ABs suggests potential clinical utility of targeted anti-BRAF therapy.
Keywords: BRAFV600E mutation; MGMT promoter hypermethylation; IDH1R132H mutant protein expression; Olig2 protein expression; astroblastoma.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures


References
-
- Bailey P, Bucy PC. Astroblastomas of the brain. Acta Psychiatr Neurol.1930;5:439–461.
-
- Aldape KD, Rosenblum MK. Astroblastoma. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, eds. WHO Classification of Tumours of the Central Nervous System. Lyon: International Agency for Research on Cancer; 2007:88–89.
-
- Bonnin JM, Rubinstein LJ. Astroblastomas: a pathological study of 23 tumors, with a postoperative follow-up in 13 patients. Neurosurgery. 1989;25 (1):6–13. - PubMed
-
- Bell JW, Osborn AG, Salzman KL et al. . Neuroradiologic characteristics of astroblastoma. Neuroradiology. 2007;49 (3):203–209. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
