

Right Unilateral Ultrabrief Pulse ECT in Geriatric Depression: Phase 1 of the PRIDE Study
- PMID: 27418379
- PMCID: PMC7130447
- DOI: 10.1176/appi.ajp.2016.15081101
Right Unilateral Ultrabrief Pulse ECT in Geriatric Depression: Phase 1 of the PRIDE Study
Abstract
Objective: The Prolonging Remission in Depressed Elderly (PRIDE) study evaluated the efficacy of right unilateral ultrabrief pulse electroconvulsive therapy (ECT) combined with venlafaxine for the treatment of geriatric depression.
Method: PRIDE was a two-phase multisite study. Phase 1 was an acute course of right unilateral ultrabrief pulse ECT, combined with open-label venlafaxine at seven academic medical centers. In phase 2 (reported separately), patients who had remitted were randomly assigned to receive pharmacotherapy (venlafaxine plus lithium) or pharmacotherapy plus continuation ECT. In phase 1, depressed patients received high-dose ECT (at six times the seizure threshold) three times per week. Venlafaxine was started during the first week of treatment and continued throughout the study. The primary outcome measure was remission, assessed with the 24-item Hamilton Depression Rating Scale (HAM-D), which was administered three times per week. Secondary outcome measures were post-ECT reorientation and safety. Paired t tests were used to estimate and evaluate the significance of change from baseline in HAM-D scores.
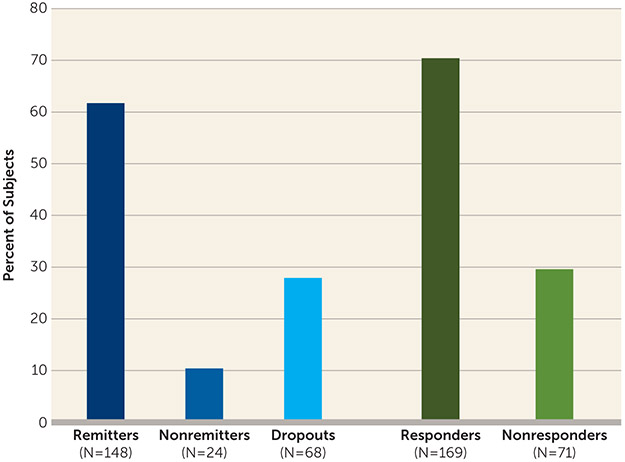
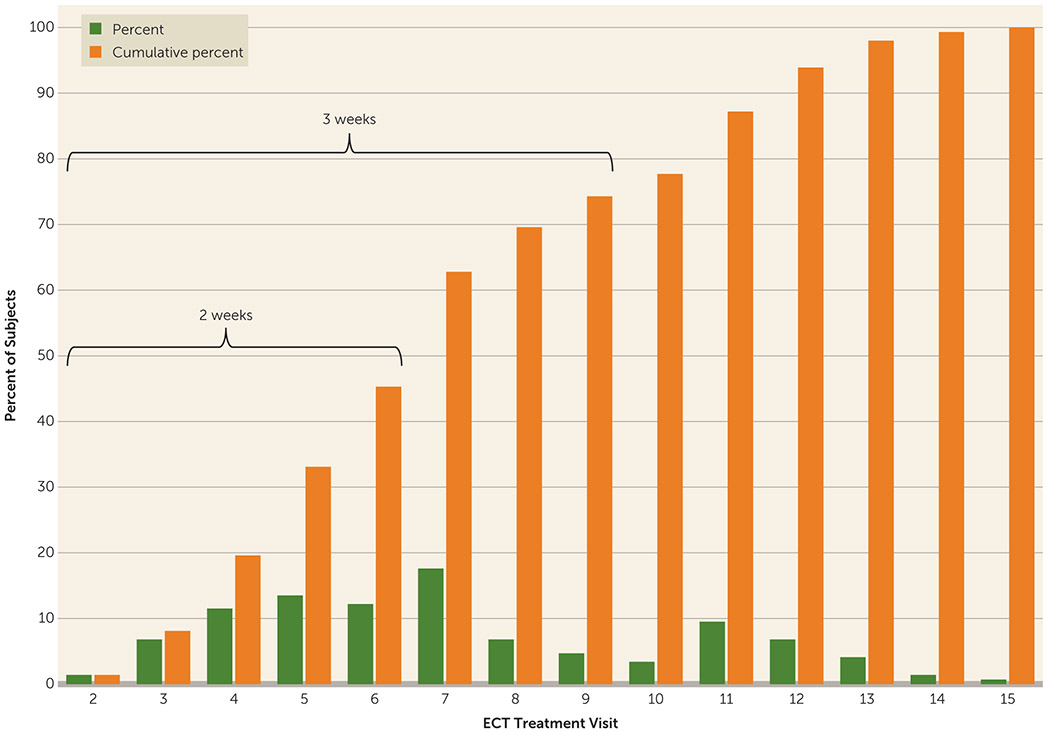
Results: Of 240 patients who entered phase 1 of the study, 172 completed it. Overall, 61.7% (148/240) of all patients met remission criteria, 10.0% (24/240) did not remit, and 28.3% (68/240) dropped out; 70% (169/240) met response criteria. Among those who remitted, the mean decrease in HAM-D score was 24.7 points (95% CI=23.4, 25.9), with a mean final score of 6.2 (SD=2.5) and an average change from baseline of 79%. The mean number of ECT treatments to remission was 7.3 (SD=3.1).
Conclusions: Right unilateral ultrabrief pulse ECT, combined with venlafaxine, is a rapidly acting and highly effective treatment option for depressed geriatric patients, with excellent safety and tolerability. These data add to the evidence base supporting the efficacy of ECT to treat severe depression in elderly patients.
Figures

Comment in
-
Evidence for the Continuing Benefits of Electroconvulsive Therapy.Am J Psychiatry. 2016 Nov 1;173(11):1071-1072. doi: 10.1176/appi.ajp.2016.16080880. Am J Psychiatry. 2016. PMID: 27799003 No abstract available.
-
Finally, Evidence for Continuation Electroconvulsive Therapy in Major Depressive Disorder.J ECT. 2016 Dec;32(4):221. doi: 10.1097/YCT.0000000000000368. J ECT. 2016. PMID: 27870658 No abstract available.
References
-
- Schulz R, Drayer RA, Rollman BL: Depression as a risk factor for non-suicide mortality in the elderly. Biol Psychiatry 2002; 52:205–225 - PubMed
-
- Conwell Y: Suicide later in life: challenges and priorities for prevention. Am J Prev Med 2014; 47(suppl 2):S244–S250 - PubMed
-
- Greenberg RM, Kellner CH: Electroconvulsive therapy: a selected review. Am J Geriatr Psychiatry 2005; 13:268–281 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
