

Clinicogenetic risk models predict early progression of follicular lymphoma after first-line immunochemotherapy
- PMID: 27418643
- PMCID: PMC5457130
- DOI: 10.1182/blood-2016-05-717355
Clinicogenetic risk models predict early progression of follicular lymphoma after first-line immunochemotherapy
Abstract
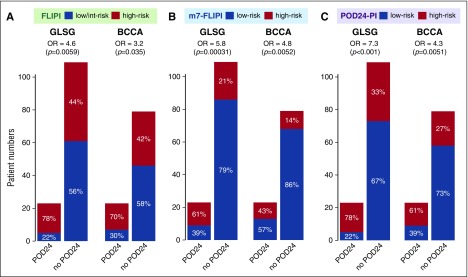
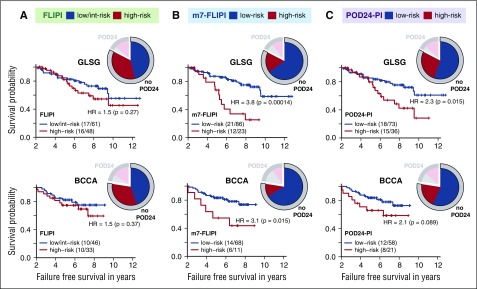
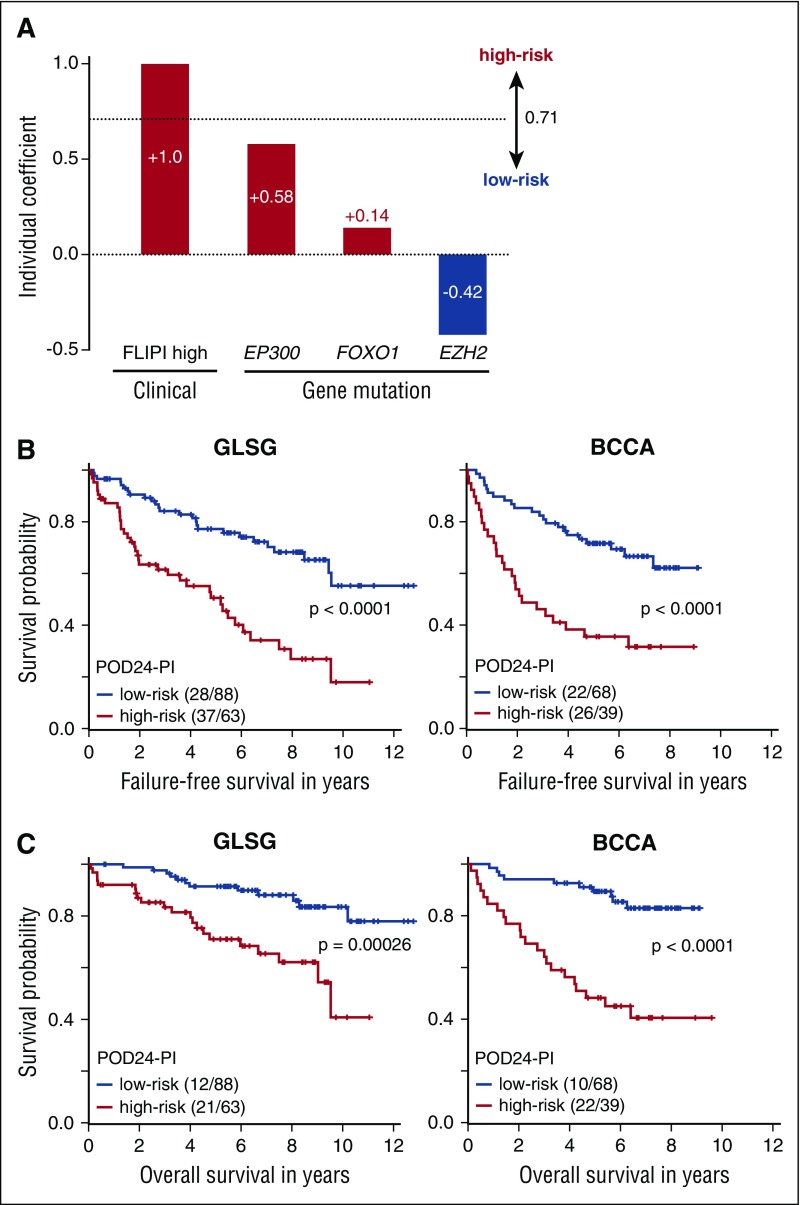
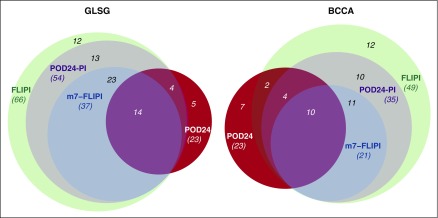
Follicular lymphoma (FL) is a clinically and molecularly heterogeneous disease. Posttreatment surrogate end points, such as progression of disease within 24 months (POD24) are promising predictors for overall survival (OS) but are of limited clinical value, primarily because they cannot guide up-front treatment decisions. We used the clinical and molecular data from 2 independent cohorts of symptomatic patients in need of first-line immunochemotherapy (151 patients from a German Low-Grade Lymphoma Study Group [GLSG] trial and 107 patients from a population-based registry of the British Columbia Cancer Agency [BCCA]) to validate the predictive utility of POD24, and to evaluate the ability of pretreatment risk models to predict early treatment failure. POD24 occurred in 17% and 23% of evaluable GLSG and BCCA patients, with 5-year OS rates of 41% (vs 91% for those without POD24, P < .0001) and 26% (vs 86%, P < .0001), respectively. The m7-FL International Prognostic Index (m7-FLIPI), a prospective clinicogenetic risk model for failure-free survival, had the highest accuracy to predict POD24 (76% and 77%, respectively) with an odds ratio of 5.82 in GLSG (P = .00031) and 4.76 in BCCA patients (P = .0052). A clinicogenetic risk model specifically designed to predict POD24, the POD24-PI, had the highest sensitivity to predict POD24, but at the expense of a lower specificity. In conclusion, the m7-FLIPI prospectively identifies the smallest subgroup of patients (28% and 22%, respectively) at highest risk of early failure of first-line immunochemotherapy and death, including patients not fulfilling the POD24 criteria, and should be evaluated in prospective trials of precision medicine approaches in FL.
© 2016 by The American Society of Hematology.
Figures

References
-
- Hiddemann W, Cheson BD. How we manage follicular lymphoma. Leukemia. 2014;28(7):1388–1395. - PubMed
-
- Mozessohn L, Cheung MC, Crump M, et al. Chemoimmunotherapy resistant follicular lymphoma: predictors of resistance, association with transformation and prognosis. Leuk Lymphoma. 2014;55(11):2502–2507. - PubMed
-
- Maurer MJ, Ghesquieres H, Ansell SM, et al. Event-free survival at 12 months (EFS12) from diagnosis is a robust endpoint for disease-related survival in patients with follicular lymphoma in the immunochemotherapy era [abstract]. Blood. 2014;124(21) Abstract 1664.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
