

Prospective Evaluation of Serum β-Glucan Testing in Patients With Probable or Proven Fungal Diseases
- PMID: 27419189
- PMCID: PMC4942764
- DOI: 10.1093/ofid/ofw128
Prospective Evaluation of Serum β-Glucan Testing in Patients With Probable or Proven Fungal Diseases
Abstract
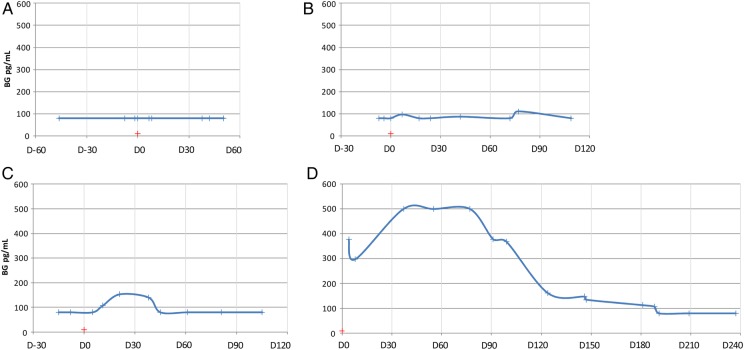
Background. Early diagnosis and treatment are crucial in invasive fungal diseases (IFD). Serum (1-3)-β-d-glucan (BG) is believed to be an early IFD marker, but its diagnostic performance has been ambiguous, with insufficient data regarding sensitivity at the time of IFD diagnosis (TOD) and according to outcome. Whether its clinical utility is equivalent for all types of IFD remains unknown. Methods. We included 143 patients with proven or probable IFD (49 invasive candidiasis, 45 invasive aspergillosis [IA], and 49 rare IFD) and analyzed serum BG (Fungitell) at TOD and during treatment. Results. (1-3)-β-d-glucan was undetectable at TOD in 36% and 48% of patients with candidemia and IA, respectively; there was no correlation between negative BG results at TOD and patients' characteristics, localization of infection, or prior antifungal use. Nevertheless, patients with candidemia due to Candida albicans were more likely to test positive for BG at TOD (odds ratio = 25.4, P = .01) than patients infected with other Candida species. In 70% of the patients with a follow-up, BG negativation occurred in >1 month for candidemia and >3 months for IA. A slower BG decrease in patients with candidemia was associated with deep-seated localizations (P = .04). Thirty-nine percent of patients with rare IFD had undetectable BG at TOD; nonetheless, all patients with chronic subcutaneous IFD tested positive at TOD. Conclusions. Undetectable serum BG does not rule out an early IFD, when the clinical suspicion is high. After IFD diagnostic, kinetics of serum BG are difficult to relate to clinical outcome.
Keywords: (1-3)-β-d-glucan; diagnostic tool; invasive fungal diseases; kinetics.
Figures
References
-
- Kontoyiannis DP, Marr KA, Park BJ et al. . Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) database. Clin Infect Dis 2010; 50:1091–100. - PubMed
-
- Pappas PG, Alexander BD, Andes DR et al. . Invasive fungal infections among organ transplant recipients: results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin Infect Dis 2010; 50:1101–11. - PubMed
-
- Pfaller MA, Diekema DJ. Epidemiology of invasive mycoses in North America. Crit Rev Microbiol 2010; 36:1–53. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
