

Variability of Post-Cardiac Arrest Care Practices Among Cardiac Arrest Centers: United States and South Korean Dual Network Survey of Emergency Physician Research Principal Investigators
- PMID: 27419613
- PMCID: PMC6913787
- DOI: 10.1089/ther.2016.0017
Variability of Post-Cardiac Arrest Care Practices Among Cardiac Arrest Centers: United States and South Korean Dual Network Survey of Emergency Physician Research Principal Investigators
Abstract
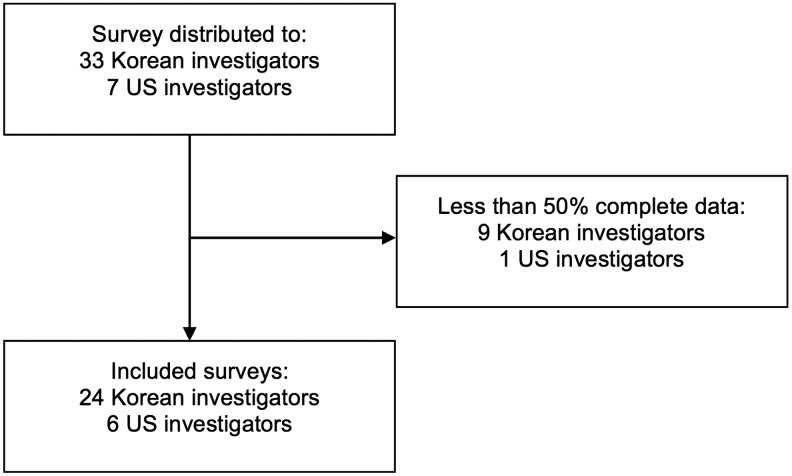
There is little consensus regarding many post-cardiac arrest care parameters. Variability in such practices could confound the results and generalizability of post-arrest care research. We sought to characterize the variability in post-cardiac arrest care practice in Korea and the United States. A 54-question survey was sent to investigators participating in one of two research groups in South Korea (Korean Hypothermia Network [KORHN]) and the United States (National Post-Arrest Research Consortium [NPARC]). Single investigators from each site were surveyed (N = 40). Participants answered questions based on local institutional protocols and practice. We calculated descriptive statistics for all variables. Forty surveys were completed during the study period with 30 having greater than 50% of questions completed (75% response rate; 24 KORHN and 6 NPARC). Most centers target either 33°C (N = 16) or vary the target based on patient characteristics (N = 13). Both bolus and continuous infusion dosing of sedation are employed. No single indication was unanimous for cardiac catheterization. Only six investigators reported having an institutional protocol for withdrawal of life-sustaining therapy (WLST). US patients with poor neurological prognosis tended to have WLST with subsequent expiration (N = 5), whereas Korean patients are transferred to a secondary care facility (N = 19). Both electroencephalography modality and duration vary between institutions. Serum biomarkers are commonly employed by Korean, but not US centers. We found significant variability in post-cardiac arrest care practices among US and Korean medical centers. These practice variations must be taken into account in future studies of post-arrest care.
Keywords: cardiac arrest; critical care neuroprognostication; targeted temperature management; therapeutic hypothermia; withdrawal of life-sustaining therapies.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Bernard S. Inducing hypothermia after out of hospital cardiac arrest. BMJ 2014;348:g2735. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med 2002;346:557–563 - PubMed
-
- Busto R, Dietrich WD, Globus MY, Ginsberg MD. Postischemic moderate hypothermia inhibits CA1 hippocampal ischemic neuronal injury. Neurosci Lett 1989;101:299–304 - PubMed
-
- Busto R, Dietrich WD, Globus MY, Valdes I, Scheinberg P, Ginsberg MD. Small differences in intraischemic brain temperature critically determine the extent of ischemic neuronal injury. J Cereb Blood Flow Metab 1987;7:729–738 - PubMed
-
- Callaway CW, Donnino MW, Fink EL, Geocadin RG, Golan E, Kern KB, Leary M, Meurer WJ, Peberdy MA, Thompson TM. Part 8: Post-cardiac arrest care: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015;132:S465–S482 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
