

Effectiveness of biomarker-based exclusion of ventilator-acquired pneumonia to reduce antibiotic use (VAPrapid-2): study protocol for a randomised controlled trial
- PMID: 27422026
- PMCID: PMC4947254
- DOI: 10.1186/s13063-016-1442-x
Effectiveness of biomarker-based exclusion of ventilator-acquired pneumonia to reduce antibiotic use (VAPrapid-2): study protocol for a randomised controlled trial
Erratum in
-
Erratum to: 'Effectiveness of biomarker-based exclusion of ventilator-acquired pneumonia to reduce antibiotic use (VAPrapid-2): study protocol for a randomised controlled trial'.Trials. 2016 Sep 26;17(1):465. doi: 10.1186/s13063-016-1594-8. Trials. 2016. PMID: 27669981 Free PMC article. No abstract available.
Abstract
Background: Ventilator-acquired pneumonia (VAP) is a common reason for antimicrobial therapy in the intensive care unit (ICU). Biomarker-based diagnostics could improve antimicrobial stewardship through rapid exclusion of VAP. Bronchoalveloar lavage (BAL) fluid biomarkers have previously been shown to allow the exclusion of VAP with high confidence.
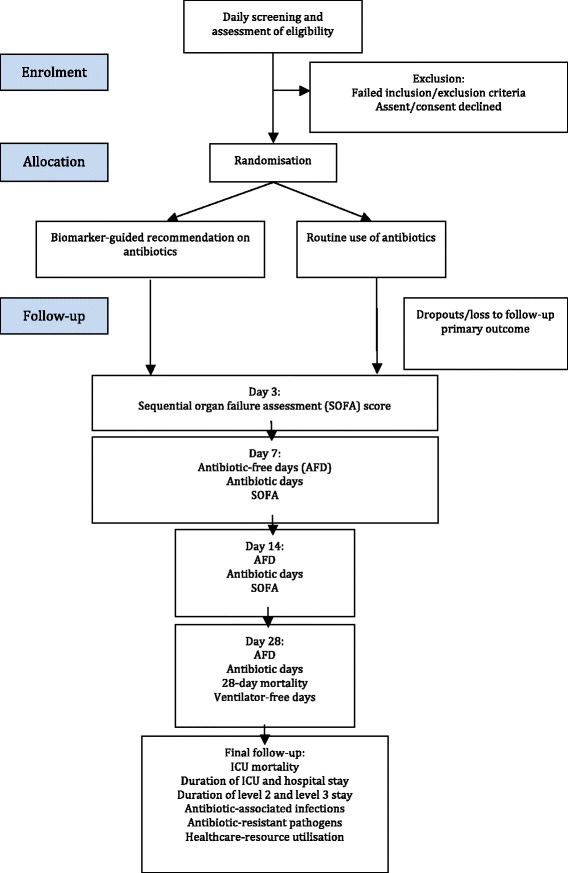
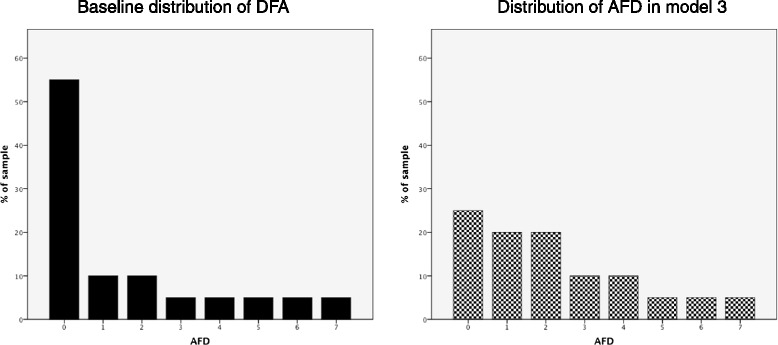
Methods/design: This is a prospective, multi-centre, randomised, controlled trial to determine whether a rapid biomarker-based exclusion of VAP results in fewer antibiotics and improved antimicrobial management. Patients with clinically suspected VAP undergo BAL, and VAP is confirmed by growth of a potential pathogen at [≥] 10(4) colony-forming units per millilitre (CFU/ml). Patients are randomised 1:1, to either a 'biomarker-guided recommendation on antibiotics' in which BAL fluid is tested for IL-1β and IL-8 in addition to routine microbiology testing, or to 'routine use of antibiotics' in which BAL undergoes routine microbiology testing only. Clinical teams are blinded to intervention until 6 hours after randomisation, when biomarker results are reported to the clinician. The primary outcome is a change in the frequency distribution of antibiotic-free days (AFD) in the 7 days following BAL. Secondary outcome measures include antibiotic use at 14 and 28 days; ventilator-free days; 28-day mortality and ICU mortality; sequential organ failure assessment (SOFA) at days 3, 7 and 14; duration of stay in critical care and the hospital; antibiotic-associated infections; and antibiotic-resistant pathogen cultures up to hospital discharge, death or 56 days. A healthcare-resource-utilisation analysis will be calculated from the duration of critical care and hospital stay. In addition, safety data will be collected with respect to performing BAL. A sample size of 210 will be required to detect a clinically significant shift in the distribution of AFD towards more patients having fewer antibiotics and therefore more AFD.
Discussion: This trial will test whether a rapid biomarker-based exclusion of VAP results in rapid discontinuation of antibiotics and therefore improves antibiotic management in patients with suspected VAP.
Trial registration: ISRCTN65937227 . Registered on 22 August 2013. ClinicalTrials.gov, NCT01972425 . Registered on 24 October 2013.
Keywords: Antibiotic stewardship; Biomarker; Randomised controlled trial; Ventilator-acquired pneumonia.
Figures
References
-
- Torres A, El-Ebiary M, Padro L, Gonzalez J, de la Bellacasa JP, Ramirez J, et al. Validation of different techniques for the diagnosis of ventilator-associated pneumonia: comparison with immediate postmortem pulmonary biopsy. Am J Respir Crit Care Med. 1994;149(2 Pt 1):324–31. doi: 10.1164/ajrccm.149.2.8306025. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
