

What are the Functional Results, Complications, and Outcomes of Using a Custom Unipolar Wrist Hemiarthroplasty for Treatment of Grade III Giant Cell Tumors of the Distal Radius?
- PMID: 27422390
- PMCID: PMC5085931
- DOI: 10.1007/s11999-016-4975-0
What are the Functional Results, Complications, and Outcomes of Using a Custom Unipolar Wrist Hemiarthroplasty for Treatment of Grade III Giant Cell Tumors of the Distal Radius?
Abstract
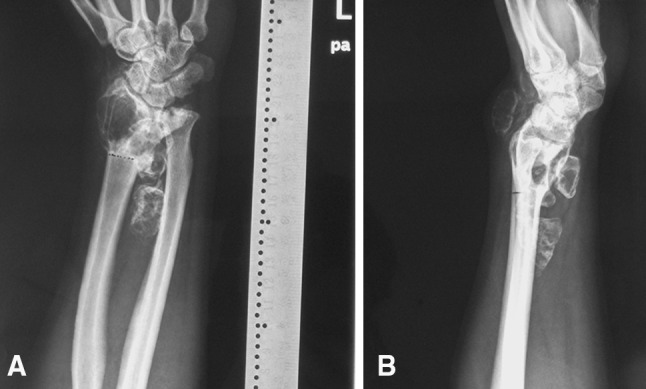
Purpose: A giant cell tumor (GCT) of bone presenting in the distal radius is rare, however, when they occur, Campanacci Grade III tumors can present formidable reconstructive challenges. They are associated with a high local recurrence rate with intralesional treatment, therefore approaches to reconstruct the wrist after en bloc resection warrant study.
Questions: We asked: (1) What are the functional outcomes after en bloc resection and reconstruction of the wrist with a unipolar prosthesis in patients with Grade III GCT of the distal radius? (2) What complications occur with use of a unipolar prosthesis in these patients? (3) What are the oncologic outcomes with using en bloc resection and reconstruction with a custom unipolar wrist hemiarthroplasty for Grade III GCTs of the distal radius?
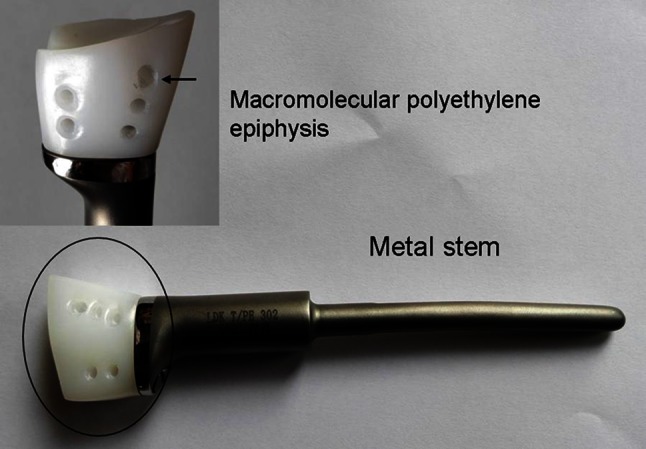
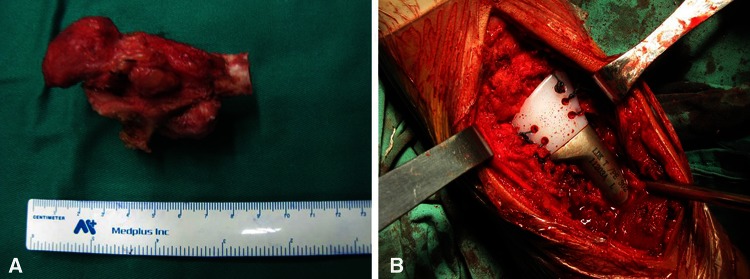
Methods: We retrospectively analyzed 10 patients with Campanacci Grade III GCTs of the distal radius treated by a unipolar prosthesis after wide resection of the tumor between January 2008 and October 2013. During that period, all patients at our medical group who presented with a Grade III GCT of the distal radius were treated with wide resection and reconstruction using a custom unipolar implant. Pre- and postoperative pain at rest were assessed according to a 10-cm VAS score. The functional outcomes of the wrist were assessed using the modified Mayo wrist score, and the degenerative changes were evaluated radiographically by a new rating system based on the Knirk and Jupiter scale. We also analyzed tumor recurrence, metastases, and complications associated with the reconstruction procedure. All patients were available for followup at a mean of 52 months (range, 24-90 months).
Results: Although the complication rate associated with prosthetic arthroplasty was relatively high (six of 10), none of our patients experienced severe complications. Two patients reported having occasional pain of the involved wrist at the time of final followup (VAS, preoperative versus postoperative: 0 versus 3; 5 versus 2, respectively). The mean modified Mayo wrist score was 68 (range, 45-90). Degenerative changes were found in three wrists (Grade 1, two patients; Grade 2, one patient). Aseptic loosening occurred in one patient and wrist subluxation occurred in two patients. Lung metastases or local tumor recurrence were not observed.
Conclusions: Because of the proportion of patients who had complications and progressive degeneration with this approach, we recommend first exploring alternatives to reconstruction with custom unipolar wrist hemiarthroplasty after resection of Grade III GCTs of the distal radius, such as fibular autografting. However, this technique provides an alternative for patients with concerns regarding possible morbidity associated with autografting, and for situations when allograft is not available.
Level of evidence: Level IV, therapeutic study.
Figures

Comment in
-
CORR ® Tumor Board: What are the Functional Results, Complications, and Outcomes of Using a Custom Unipolar Wrist Hemiarthroplasty for Treatment of Grade III Giant Cell Tumors of the Distal Radius?Clin Orthop Relat Res. 2016 Dec;474(12):2580-2582. doi: 10.1007/s11999-016-5076-9. Epub 2016 Sep 13. Clin Orthop Relat Res. 2016. PMID: 27623785 Free PMC article. No abstract available.
-
CORR Insights®: What are the Functional Results, Complications, and Outcomes of Using a Custom Unipolar Wrist Hemiarthroplasty for Treatment of Grade III Giant Cell Tumors of the Distal Radius?Clin Orthop Relat Res. 2016 Dec;474(12):2591-2593. doi: 10.1007/s11999-016-5052-4. Epub 2016 Sep 13. Clin Orthop Relat Res. 2016. PMID: 27623786 Free PMC article. No abstract available.
Similar articles
-
Does Wrist Arthrodesis With Structural Iliac Crest Bone Graft After Wide Resection of Distal Radius Giant Cell Tumor Result in Satisfactory Function and Local Control?Clin Orthop Relat Res. 2017 Mar;475(3):767-775. doi: 10.1007/s11999-015-4678-y. Clin Orthop Relat Res. 2017. PMID: 26728519 Free PMC article.
-
The functional outcomes and complications of different reconstruction methods for Giant cell tumor of the distal radius: comparison of Osteoarticular allograft and three-dimensional-printed prosthesis.BMC Musculoskelet Disord. 2020 Feb 3;21(1):69. doi: 10.1186/s12891-020-3084-0. BMC Musculoskelet Disord. 2020. PMID: 32013950 Free PMC article.
-
Functional outcome of en bloc excision and custom prosthetic replacement for giant cell tumor of the distal radius.J Orthop Sci. 2015 Nov;20(6):1090-7. doi: 10.1007/s00776-015-0763-z. Epub 2015 Sep 2. J Orthop Sci. 2015. PMID: 26329932
-
En bloc excision and customized prosthesis replacement for Campanacci III giant cell tumours of the distal radius: five cases report and a review of the literature.BMC Musculoskelet Disord. 2025 Jul 4;26(1):617. doi: 10.1186/s12891-025-08851-1. BMC Musculoskelet Disord. 2025. PMID: 40615999 Free PMC article. Review.
-
En bloc excision and autogenous fibular reconstruction for aggressive giant cell tumor of distal radius: a report of 12 cases and review of literature.J Orthop Surg Res. 2011 Mar 8;6:14. doi: 10.1186/1749-799X-6-14. J Orthop Surg Res. 2011. PMID: 21385393 Free PMC article. Review.
Cited by
-
Management of giant cell tumors of the distal radius.J Orthop. 2023 Jun 2;41:47-56. doi: 10.1016/j.jor.2023.06.001. eCollection 2023 Jul. J Orthop. 2023. PMID: 37324809 Free PMC article.
-
Current Concepts in the Treatment of Giant Cell Tumor of Bone: An Update.Curr Oncol. 2024 Apr 8;31(4):2112-2132. doi: 10.3390/curroncol31040157. Curr Oncol. 2024. PMID: 38668060 Free PMC article. Review.
-
Surgical challenges, novel techniques, and systemic treatment of giant cell tumour of bone of the distal radius : clinical outcomes and systematic review of the literature.Bone Jt Open. 2022 Jul;3(7):515-528. doi: 10.1302/2633-1462.37.BJO-2022-0064.R1. Bone Jt Open. 2022. PMID: 35775196 Free PMC article.
-
Customized Metal 3D Printed Total Wrist Prosthesis in the Treatment of Severely Destroyed Wrist: Design Rationale and Clinical Applications.Orthop Surg. 2025 May;17(5):1536-1546. doi: 10.1111/os.70030. Epub 2025 Mar 26. Orthop Surg. 2025. PMID: 40135373 Free PMC article.
-
Intercalary reconstruction with successful joint preservation by uncemented 3D‑printed endoprosthesis following tumor resection in distal radius: A case report.Exp Ther Med. 2022 Oct 17;24(6):719. doi: 10.3892/etm.2022.11655. eCollection 2022 Dec. Exp Ther Med. 2022. PMID: 36340601 Free PMC article.
References
-
- Abat F, Almenara M, Peiro A, Trullols L, Bague S, Gracia I. Giant cell tumour of bone: a series of 97 cases with a mean follow-up of 12 years. Rev Esp Cir Ortop Traumatol. 2015;59:59–65. - PubMed
-
- Bassiony AA. Giant cell tumour of the distal radius: wide resection and reconstruction by non-vascularised proximal fibular autograft. Ann Acad Med Singapore. 2009;38:900–904. - PubMed
-
- Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. J Bone Joint Surg Am. 1987;69:106–114. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
