

Pain Mechanisms and Centralized Pain in Temporomandibular Disorders
- PMID: 27422858
- PMCID: PMC5004242
- DOI: 10.1177/0022034516657070
Pain Mechanisms and Centralized Pain in Temporomandibular Disorders
Abstract
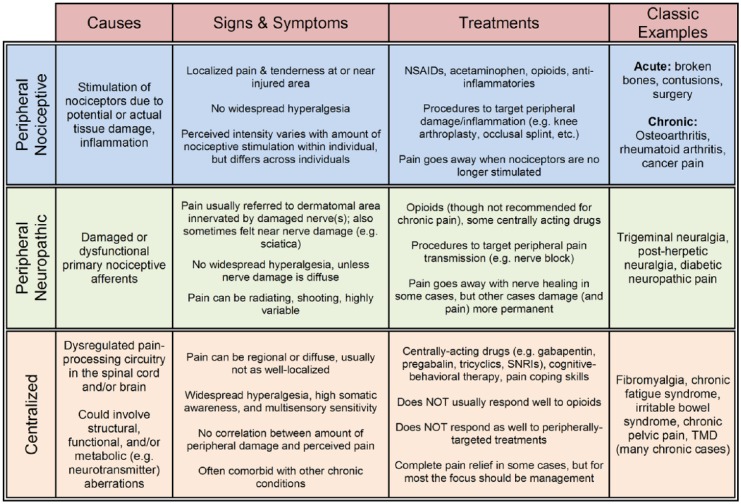
Until recently, most clinicians and scientists believed that the experience of pain is perceptually proportional to the amount of incoming peripheral nociceptive drive due to injury or inflammation in the area perceived to be painful. However, many cases of chronic pain have defied this logic, leaving clinicians perplexed as to how patients are experiencing pain with no obvious signs of injury in the periphery. Conversely, there are patients who have a peripheral injury and/or inflammation but little or no pain. What makes some individuals experience intense pain with minimal peripheral nociceptive stimulation and others experience minimal pain with serious injury? It is increasingly well accepted in the scientific community that pain can be generated and maintained or, through other mechanisms, suppressed by changes in the central nervous system, creating a complete mismatch between peripheral nociceptive drive and perceived pain. In fact, there is no known chronic pain condition where the observed extent of peripheral damage reproducibly engenders the same level of pain across individuals. Temporomandibular disorders (TMDs) are no exception. This review focuses on the idea that TMD patients range on a continuum-from those whose pain is generated peripherally to those whose pain is centralized (i.e., generated, exacerbated, and/or maintained by central nervous system mechanisms). This article uses other centralized chronic pain conditions as a guide, and it suggests that the mechanistic variability in TMD pain etiology has prevented us from adequately treating many individuals who are diagnosed with the condition. As the field moves forward, it will be imperative to understand each person's pain from its own mechanistic standpoint, which will enable clinicians to deliver personalized medicine to TMD patients and eventually provide relief in even the most recalcitrant cases.
Keywords: evidence-based dentistry/health care; multisensory perception; neuroscience/ neurobiology; orofacial pain/TMD; psychosocial factors; treatment planning.
© International & American Associations for Dental Research 2016.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Figures
Similar articles
-
The Neurobiology of Orofacial Pain and Sleep and Their Interactions.J Dent Res. 2016 Sep;95(10):1109-16. doi: 10.1177/0022034516648264. Epub 2016 May 6. J Dent Res. 2016. PMID: 27154736 Review.
-
Chronicity factors of temporomandibular disorders: a critical review of the literature.Braz Oral Res. 2015;29:S1806-83242015000100300. doi: 10.1590/1807-3107BOR-2015.vol29.0018. Epub 2015 Jan 13. Braz Oral Res. 2015. PMID: 25590505 Review.
-
Diagnosing and treating chronic musculoskeletal pain based on the underlying mechanism(s).Best Pract Res Clin Rheumatol. 2015 Feb;29(1):6-19. doi: 10.1016/j.berh.2015.04.024. Epub 2015 May 23. Best Pract Res Clin Rheumatol. 2015. PMID: 26266995 Review.
-
TMD and chronic pain: a current view.Dental Press J Orthod. 2015 Jan-Feb;20(1):127-33. doi: 10.1590/2176-9451.20.1.127-133.sar. Dental Press J Orthod. 2015. PMID: 25741834 Free PMC article. Review.
-
Why look in the brain for answers to temporomandibular disorder pain?Cells Tissues Organs. 2005;180(1):69-75. doi: 10.1159/000086200. Cells Tissues Organs. 2005. PMID: 16088135 Review.
Cited by
-
Temporomandibular disorders cases with high-impact pain are more likely to experience short-term pain fluctuations.Sci Rep. 2022 Jan 31;12(1):1657. doi: 10.1038/s41598-022-05598-w. Sci Rep. 2022. PMID: 35102207 Free PMC article.
-
Administration of low-level laser on muscles of mastication following the induction of initial fatigue: protocol for a randomized, controlled, clinical trial.Medicine (Baltimore). 2018 Jun;97(26):e11340. doi: 10.1097/MD.0000000000011340. Medicine (Baltimore). 2018. PMID: 29953026 Free PMC article. Clinical Trial.
-
ICD-10 Codes for the Study of Chronic Overlapping Pain Conditions in Administrative Databases.J Pain. 2020 Jan-Feb;21(1-2):59-70. doi: 10.1016/j.jpain.2019.05.007. Epub 2019 May 30. J Pain. 2020. PMID: 31154033 Free PMC article.
-
Perspective: Advancing the science regarding temporomandibular disorders.Front Dent Med. 2024 May 16;5:1374883. doi: 10.3389/fdmed.2024.1374883. eCollection 2024. Front Dent Med. 2024. PMID: 39917712 Free PMC article.
-
Analgesic effects of the CTK 01512-2 toxin in different models of orofacial pain in rats.Pharmacol Rep. 2020 Jun;72(3):600-611. doi: 10.1007/s43440-020-00108-z. Epub 2020 May 12. Pharmacol Rep. 2020. PMID: 32399819
References
-
- Aaron LA, Burke MM, Buchwald D. 2000. Overlapping conditions among patients with chronic fatigue syndrome, fibromyalgia, and temporomandibular disorder. Arch Intern Med. 160(2):221–227. - PubMed
-
- Ablin JN, Buskila D, Clauw DJ. 2009. Biomarkers in fibromyalgia. Curr Pain Headache Rep. 13(5):343–349. - PubMed
-
- Ablin K, Clauw DJ. 2009. From fibrositis to functional somatic syndromes to a bell-shaped curve of pain and sensory sensitivity: evolution of a clinical construct. Rheum Dis Clin North Am. 35(2):233–251. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
