

Endothelial hyperpermeability in severe pulmonary arterial hypertension: role of store-operated calcium entry
- PMID: 27422996
- PMCID: PMC5142214
- DOI: 10.1152/ajplung.00057.2016
Endothelial hyperpermeability in severe pulmonary arterial hypertension: role of store-operated calcium entry
Abstract
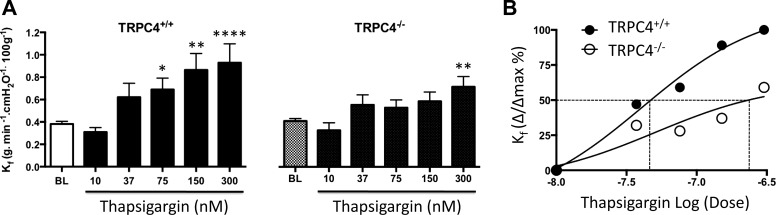
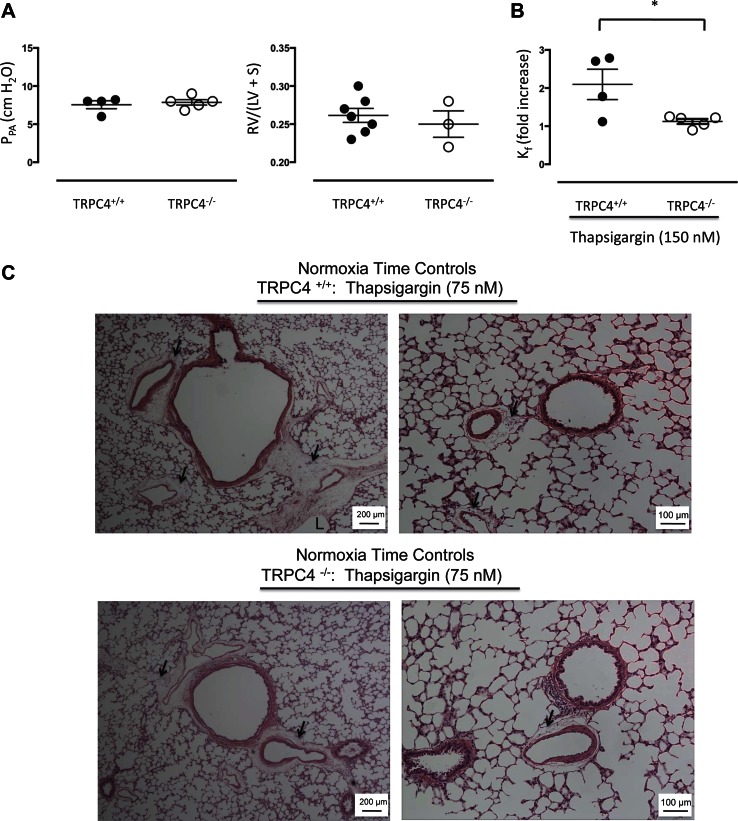
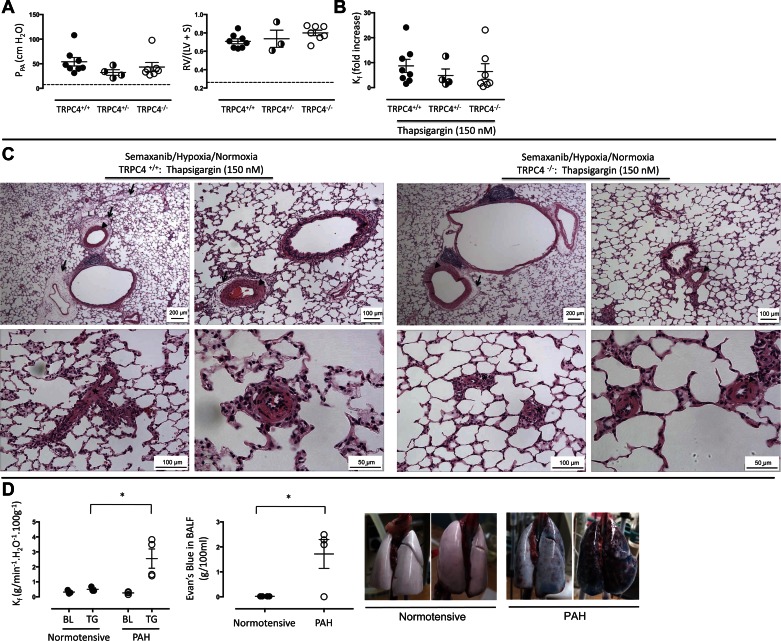
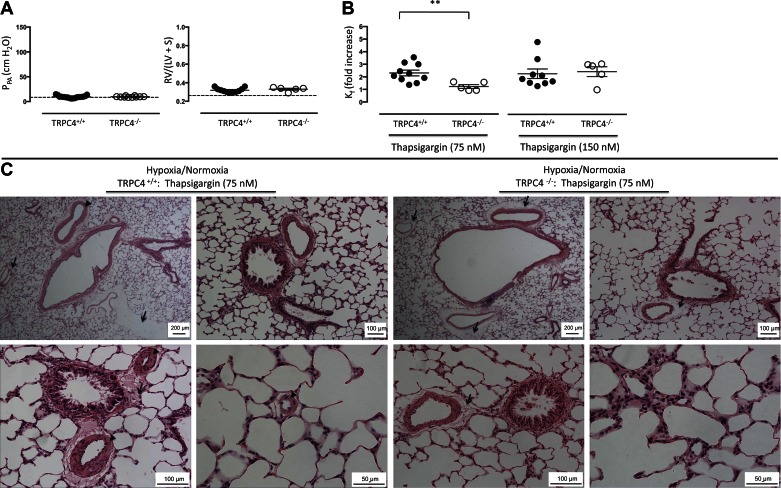
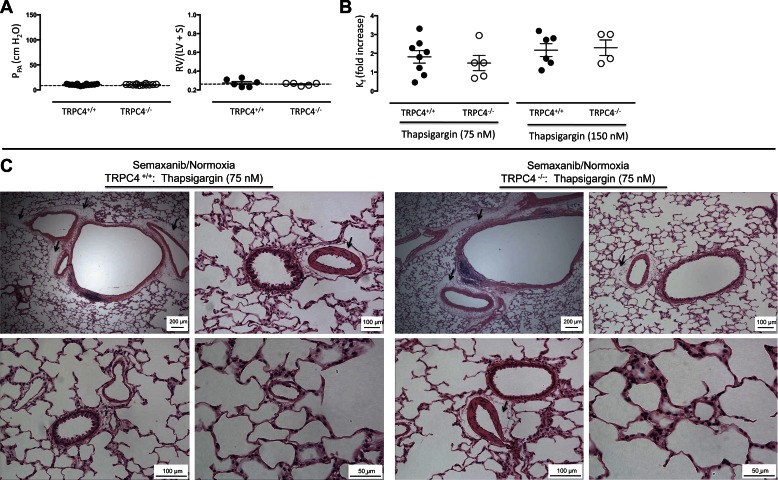
Here, we tested the hypothesis that animals with severe pulmonary arterial hypertension (PAH) display increased sensitivity to vascular permeability induced by activation of store-operated calcium entry. To test this hypothesis, wild-type and transient receptor potential channel 4 (TRPC4) knockout Fischer 344 rats were given a single injection of Semaxanib (SU5416; 20 mg/kg) followed by 3 wk of exposure to hypoxia (10% oxygen) and a return to normoxia (21% oxygen) for an additional 2-3 wk. This Semaxanib/hypoxia/normoxia (i.e., SU5416/hypoxia/normoxia) treatment caused PAH, as evidenced by development of right ventricular hypertrophy, pulmonary artery medial hypertrophy, and occlusive lesions within precapillary arterioles. Pulmonary artery pressure was increased fivefold in Semaxanib/hypoxia/normoxia-treated animals compared with untreated, Semaxanib-treated, and hypoxia-treated controls, determined by isolated perfused lung studies. Thapsigargin induced a dose-dependent increase in permeability that was dependent on TRPC4 in the normotensive perfused lung. This increase in permeability was accentuated in PAH lungs but not in Semaxanib- or hypoxia-treated lungs. Fluid accumulated in large perivascular cuffs, and although alveolar fluid accumulation was not seen in histological sections, Evans blue dye conjugated to albumin was present in bronchoalveolar lavage fluid of hypertensive but not normotensive lungs. Thus PAH is accompanied by a TRPC4-dependent increase in the sensitivity to edemagenic agents that activate store-operated calcium entry.
Keywords: Semaxanib; Sugen 5416; TRPC4; calcium channels; canonical transient receptor potential 4; edema; filtration coefficient.
Copyright © 2016 the American Physiological Society.
Figures
Similar articles
-
TRPC4 inactivation confers a survival benefit in severe pulmonary arterial hypertension.Am J Pathol. 2013 Dec;183(6):1779-1788. doi: 10.1016/j.ajpath.2013.08.016. Epub 2013 Oct 8. Am J Pathol. 2013. PMID: 24113457 Free PMC article.
-
Transient Receptor Potential Channel 4 Encodes a Vascular Permeability Defect and High-Frequency Ca(2+) Transients in Severe Pulmonary Arterial Hypertension.Am J Pathol. 2016 Jun;186(6):1701-9. doi: 10.1016/j.ajpath.2016.02.002. Epub 2016 Apr 12. Am J Pathol. 2016. PMID: 27083517 Free PMC article.
-
The role of endothelial leak in pulmonary hypertension (2017 Grover Conference Series).Pulm Circ. 2018 Oct-Dec;8(4):2045894018798569. doi: 10.1177/2045894018798569. Epub 2018 Aug 20. Pulm Circ. 2018. PMID: 30124139 Free PMC article.
-
Role of Ca2+ signaling in the regulation of endothelial permeability.Vascul Pharmacol. 2002 Nov;39(4-5):173-85. doi: 10.1016/s1537-1891(03)00007-7. Vascul Pharmacol. 2002. PMID: 12747958 Review.
-
Ca2+ signaling, TRP channels, and endothelial permeability.Microcirculation. 2006 Dec;13(8):693-708. doi: 10.1080/10739680600930347. Microcirculation. 2006. PMID: 17085428 Review.
Cited by
-
Inflammation in Pulmonary Arterial Hypertension.Adv Exp Med Biol. 2021;1303:351-372. doi: 10.1007/978-3-030-63046-1_19. Adv Exp Med Biol. 2021. PMID: 33788202 Review.
-
Spontaneous pulmonary hypertension in genetic mouse models of natural killer cell deficiency.Am J Physiol Lung Cell Mol Physiol. 2018 Dec 1;315(6):L977-L990. doi: 10.1152/ajplung.00477.2017. Epub 2018 Sep 20. Am J Physiol Lung Cell Mol Physiol. 2018. PMID: 30234375 Free PMC article.
-
Biventricular diastolic dysfunction, thrombocytopenia, and red blood cell macrocytosis in experimental pulmonary arterial hypertension.Pulm Circ. 2020 May 26;10(2):2045894020908787. doi: 10.1177/2045894020908787. eCollection 2020 Apr-Jun. Pulm Circ. 2020. PMID: 32518619 Free PMC article.
-
Current Overview of the Biology and Pharmacology in Sugen/Hypoxia-Induced Pulmonary Hypertension in Rats.J Aerosol Med Pulm Drug Deliv. 2024 Oct;37(5):241-283. doi: 10.1089/jamp.2024.0016. J Aerosol Med Pulm Drug Deliv. 2024. PMID: 39388691 Review.
-
Mitochondrial dysfunction and pulmonary hypertension: cause, effect, or both.Am J Physiol Lung Cell Mol Physiol. 2018 May 1;314(5):L782-L796. doi: 10.1152/ajplung.00331.2017. Epub 2018 Jan 18. Am J Physiol Lung Cell Mol Physiol. 2018. PMID: 29345195 Free PMC article. Review.
References
-
- Abe K, Toba M, Alzoubi A, Ito M, Fagan KA, Cool CD, Voelkel NF, McMurtry IF, Oka M. Formation of plexiform lesions in experimental severe pulmonary arterial hypertension. Circulation 121: 2747–2754, 2010. - PubMed
-
- Alvarez DF, Gjerde EA, Townsley MI. Role of EETs in regulation of endothelial permeability in rat lung. Am J Physiol Lung Cell Mol Physiol 286: L445–L451, 2004. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical