

[Effectiveness and economic impact of a program of integrated care with telemedicine support on insulin-treated type 2 diabetic patients (Study GITDIABE)]
- PMID: 27423246
- PMCID: PMC6876025
- DOI: 10.1016/j.aprim.2016.04.004
[Effectiveness and economic impact of a program of integrated care with telemedicine support on insulin-treated type 2 diabetic patients (Study GITDIABE)]
Abstract
Aim: To evaluate if insulin-treated type 2 diabetic patients with blood glucose self-monitoring (DIA), included in a program of integrated management of diabetes mellitus (DM), achieve a better level of metabolic control with telemedicine support than with conventional support, after 12 months follow-up. The impact on the use and cost of healthcare services, pharmaceutical expenditure, and consumption of test strips for blood glucose, was also assessed.
Design: A prospective parallel cohorts study.
Field: Four basic health areas of an integrated healthcare organisation.
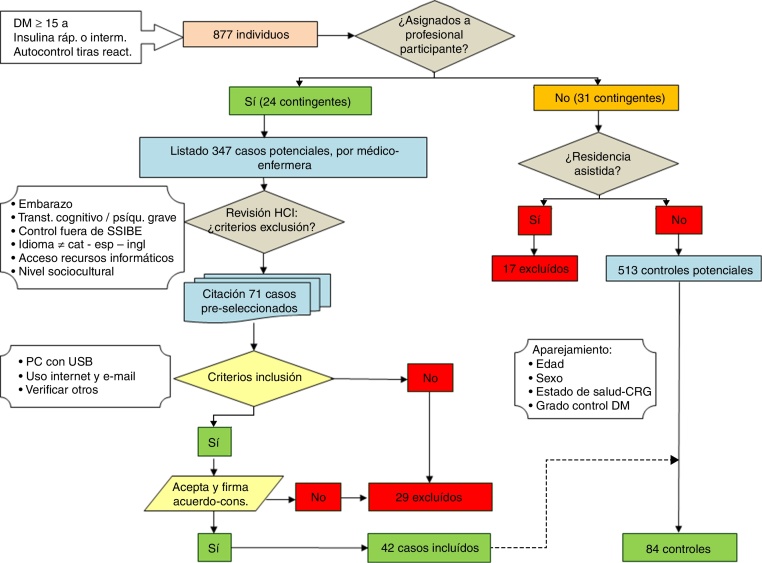
Participants: The study included 126 DIA patients aged 15 or more years, treated with rapid or intermediate Insulin and blood glucose self-monitoring, grouped into 42 cases and 84 controls, matched according to age, sex, level of metabolic control, and morbidity profile.
Intervention: Telematics physician-patient communication and download of blood glucose self-monitoring data through the Emminens eConecta® platform; test strips home delivered according to consumption. Hidden controls with usual follow-up.
Main measurements: Glycosylated haemoglobin (%HbA1c); perception of quality of life (EuroQol-5 and EsDQOL); cardiovascular risk; use of healthcare resources; consumption of test strips; pharmaceutical and healthcare expenditure.
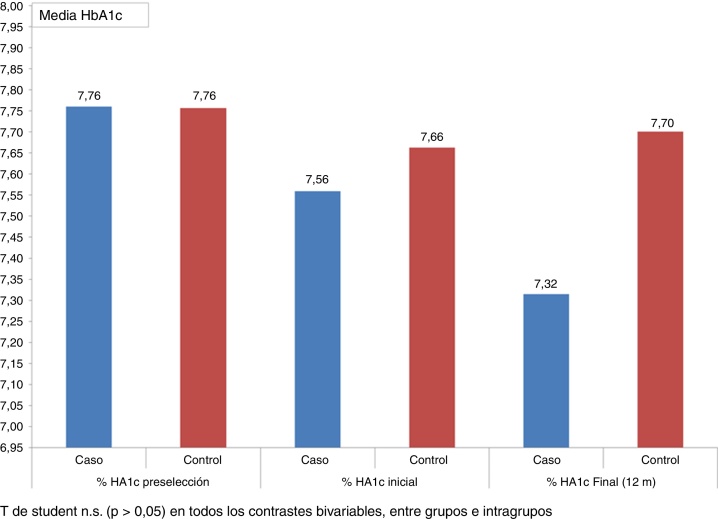
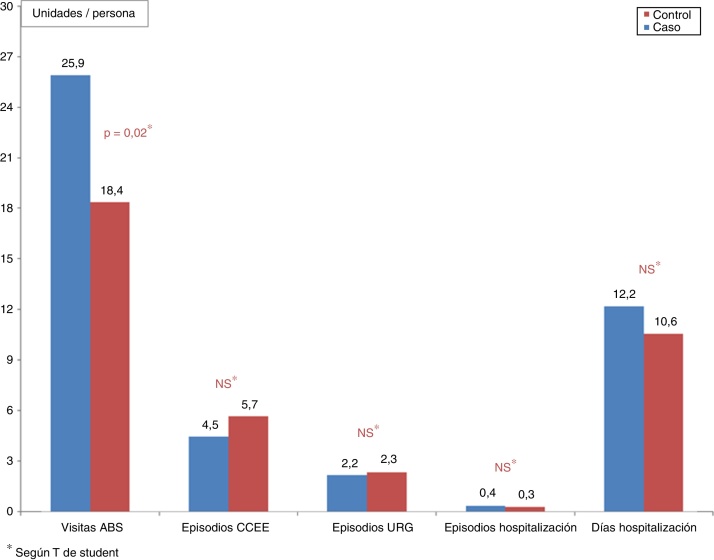
Results: Reduction of 0.38% in HbA1c in the cases (95% CI:-0.89% to 0.12%). No significant differences with regard to any of the activities registered, or any significant change in the quality of life.
Conclusions: The results obtained are similar to other equivalent studies. The profile of the patient is elderly and with multiple morbidities, who still have technological limitations. To surpass these barriers, it would be necessary to devote more time to the training and to the resolution of possible technological problems.
Objetivo: Evaluar si pacientes diabéticos tipo 2 con insulina y autocontrol (DIA) incluidos en un programa de gestión integrada de la diabetes mellitus (DM) con seguimiento telemático alcanzan un grado de control metabólico a los 12 meses mejor que los no incluidos, así como el impacto en la utilización y el coste de servicios sanitarios, consumo de fármacos y tiras reactivas.
Diseño: Estudio prospectivo de cohortes paralelas.
Emplazamiento: Cuatro áreas básicas de salud de una organización sanitaria integrada.
Participantes: Ciento veintiséis pacientes DIA de 15 o más años en tratamiento con insulina rápida o intermedia con autocontroles: 42 casos y 84 controles emparejados según edad, sexo, grado de control de la DM y perfil de morbilidad.
Intervención: Comunicación telemática médico-paciente y volcado de glucemias mediante la plataforma Emminens eConecta®; suministro a domicilio de tiras reactivas según consumo. Controles ocultos, con seguimiento habitual.
Mediciones principales: Hemoglobina glucosilada (% HbA1c); percepción de calidad de vida (EuroQol-5 y EsDQOL); riesgo cardiovascular; utilización de recursos sanitarios; consumo de tiras reactivas y medicamentos; gasto sanitario total.
Resultados: Reducción de %HbA1c en casos respecto a controles de 0,38% (IC95% −0,89% a 0,12%). Sin diferencias significativas respecto a ninguna de las actividades registradas, ni cambios significativos en la calidad de vida.
Conclusiones: Los resultados obtenidos no difieren de otros estudios equiparables. El perfil es de un paciente anciano y pluripatológico que tiene todavía limitaciones tecnológicas. Para superar estas barreras se debería dedicar más tiempo a la formación y a la resolución de problemas tecnológicos.
Keywords: Automonitorización de la glucosa sanguínea; Blood glucose self-monitoring; Calidad de vida; Diabetes mellitus; Quality of life; Telemedicina; Telemedicine.
Copyright © 2016 Elsevier España, S.L.U. All rights reserved.
Figures
References
-
- Inzucchi S.E., Bergenstal R.M., Buse J.B., Diamant M., Ferrannini E., Nauck M. Management of hyperglycaemia in type 2 diabetes: A patient-centered approach. Position statement of the american diabetes association (ADA) and the european association for the study of diabetes (EASD) Diabetologia. 2012;55:1577–1596. - PubMed
-
- Ceriello A., Barkai L., Christiansen J.S., Czupryniak L., Gomis R., Harno K. Diabetes as a case study of chronic disease management with a personalized approach: The role of a structured feedback loop. Diabetes Res Clin Pract. 2012;98:5–10. - PubMed
-
- Picón-César M.J. Documento de posicionamiento sobre el uso de la telemedicina aplicada a la atención diabetológica. Av Diabetol. 2010;26:147–150.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
