

Relapse patterns and outcome after relapse in standard risk medulloblastoma: a report from the HIT-SIOP-PNET4 study
- PMID: 27423645
- PMCID: PMC5020107
- DOI: 10.1007/s11060-016-2202-1
Relapse patterns and outcome after relapse in standard risk medulloblastoma: a report from the HIT-SIOP-PNET4 study
Abstract
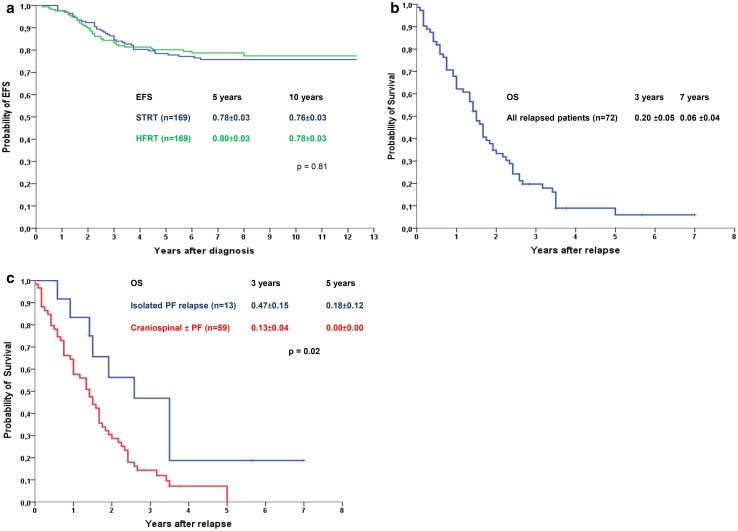
The HIT-SIOP-PNET4 randomised trial for standard risk medulloblastoma (MB) (2001-2006) included 338 patients and compared hyperfractionated and conventional radiotherapy. We here report the long-term outcome after a median follow up of 7.8 years, including detailed information on relapse and the treatment of relapse. Data were extracted from the HIT Group Relapsed MB database and by way of a specific case report form. The event-free and overall (OS) survival at 10 years were 76 ± 2 % and 78 ± 2 % respectively with no significant difference between the treatment arms. Seventy-two relapses and three second malignant neoplasms were reported. Thirteen relapses (18 %) were isolated local relapses in the posterior fossa (PF) and 59 (82 %) were craniospinal, metastatic relapses (isolated or multiple) with or without concurrent PF disease. Isolated PF relapse vs all other relapses occurred at mean/median of 38/35 and 28/26 months respectively (p = 0.24). Late relapse, i.e. >5 years from diagnosis, occurred in six patients (8 %). Relapse treatment consisted of combinations of surgery (25 %), focal radiotherapy (RT 22 %), high dose chemotherapy with stem cell rescue (HDSCR 21 %) and conventional chemotherapy (90 %). OS at 5 years after relapse was 6.0 ± 4 %. In multivariate analysis; isolated relapse in PF, and surgery were significantly associated with prolonged survival whereas RT and HDSCR were not. Survival after relapse was not related to biological factors and was very poor despite several patients receiving intensive treatments. Exploration of new drugs is warranted, preferably based on tumour biology from biopsy of the relapsed tumour.
Keywords: Chemotherapy; Clinical trial; Medulloblastoma; Paediatric; Radiotherapy; Relapse; Secondary tumours; Survival; Treatment.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Lannering B, Rutkowski S, Doz F, Pizer B, Gustafsson G, Navajas A, Massimino M, Reddingius R, Benesch M, Carrie C, Taylor R, Gandola L, Bjork-Eriksson T, Giralt J, Oldenburger F, Pietsch T, Figarella-Branger D, Robson K, Forni M, Clifford SC, Warmuth-Metz M, von Hoff K, Faldum A, Mosseri V, Kortmann R. Hyperfractionated versus conventional radiotherapy followed by chemotherapy in standard-risk medulloblastoma: results from the randomized multicenter HIT-SIOP PNET 4 trial. J Clin Oncol. 2012;30:3187–3193. doi: 10.1200/JCO.2011.39.8719. - DOI - PubMed
-
- Bouffet E, Doz F, Demaille MC, Tron P, Roche H, Plantaz D, Thyss A, Stephan JL, Lejars O, Sariban E, Buclon M, Zucker JM, Brunat-Mentigny M, Bernard JL, Gentet JC. Improving survival in recurrent medulloblastoma: earlier detection, better treatment or still an impasse? Br J Cancer. 1998;77:1321–1326. doi: 10.1038/bjc.1998.220. - DOI - PMC - PubMed
-
- Bode U, Zimmermann M, Moser O, Rutkowski S, Warmuth-Metz M, Pietsch T, Kortmann RD, Faldum A, Fleischhack G. Treatment of recurrent primitive neuroectodermal tumors (PNET) in children and adolescents with high-dose chemotherapy (HDC) and stem cell support: results of the HITREZ 97 multicentre trial. J Neurooncol. 2014;120:635–642. doi: 10.1007/s11060-014-1598-8. - DOI - PubMed
-
- Hill RM, Kuijper S, Lindsey JC, Petrie K, Schwalbe EC, Barker K, Boult JK, Williamson D, Ahmad Z, Hallsworth A, Ryan SL, Poon E, Robinson SP, Ruddle R, Raynaud FI, Howell L, Kwok C, Joshi A, Nicholson SL, Crosier S, Ellison DW, Wharton SB, Robson K, Michalski A, Hargrave D, Jacques TS, Pizer B, Bailey S, Swartling FJ, Weiss WA, Chesler L, Clifford SC. Combined MYC and P53 defects emerge at medulloblastoma relapse and define rapidly progressive, therapeutically targetable disease. Cancer Cell. 2015;27:72–84. doi: 10.1016/j.ccell.2014.11.002. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
