

Implementing PGD/PGD-A in IVF clinics: considerations for the best laboratory approach and management
- PMID: 27423665
- PMCID: PMC5065548
- DOI: 10.1007/s10815-016-0768-3
Implementing PGD/PGD-A in IVF clinics: considerations for the best laboratory approach and management
Abstract
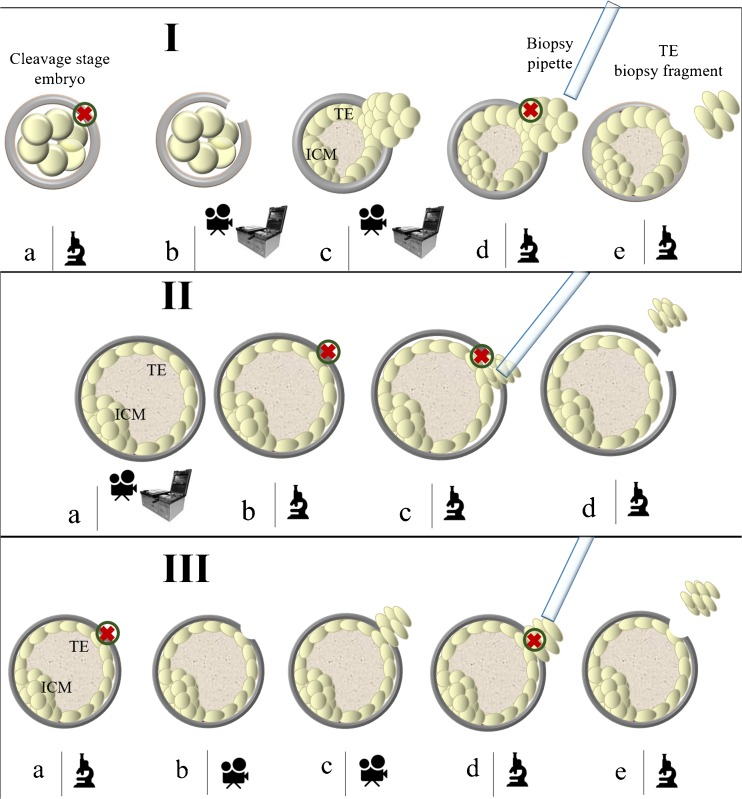
For an IVF clinic that wishes to implement preimplantation genetic diagnosis for monogenic diseases (PGD) and for aneuploidy testing (PGD-A), a global improvement is required through all the steps of an IVF treatment and patient care. At present, CCS (Comprehensive Chromosome Screening)-based trophectoderm (TE) biopsy has been demonstrated as a safe, accurate and reproducible approach to conduct PGD-A and possibly also PGD from the same biopsy. Key challenges in PGD/PGD-A implementation cover genetic and reproductive counselling, selection of the most efficient approach for blastocyst biopsy as well as of the best performing molecular technique to conduct CCS and monogenic disease analysis. Three different approaches for TE biopsy can be compared. However, among them, the application of TE biopsy approaches, entailing the zona opening when the expanded blastocyst stage is reached, represent the only biopsy methods suited with a totally undisturbed embryo culture strategy (time lapse-based incubation in a single media). Moreover, contemporary CCS technologies show a different spectrum of capabilities and limits that potentially impact the clinical outcomes, the management and the applicability of the PGD-A itself. In general, CCS approaches that avoid the use of whole genome amplification (WGA) can provide higher reliability of results with lower costs and turnaround time of analysis. The future perspectives are focused on the scrupulous and rigorous clinical validations of novel CCS methods based on targeted approaches that avoid the use of WGA, such as targeted next-generation sequencing technology, to further improve the throughput of analysis and the overall cost-effectiveness of PGD/PGD-A.
Keywords: CCS; Embryo selection; PGD; PGD-A; PGS; Trophectoderm biopsy.
Figures
References
-
- Dahdouh EM, Balayla J, Audibert F, Genetics Committee. Wilson RD, Audibert F, Brock JA, Campagnolo C, Carroll J, Chong K, Gagnon A, Johnson JA, MacDonald W, Okun N, Pastuck M, Vallée-Pouliot K. Technical update: preimplantation genetic diagnosis and screening. J Obstet Gynaecol Can. 2015;37(5):451–63. doi: 10.1016/S1701-2163(15)30261-9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
